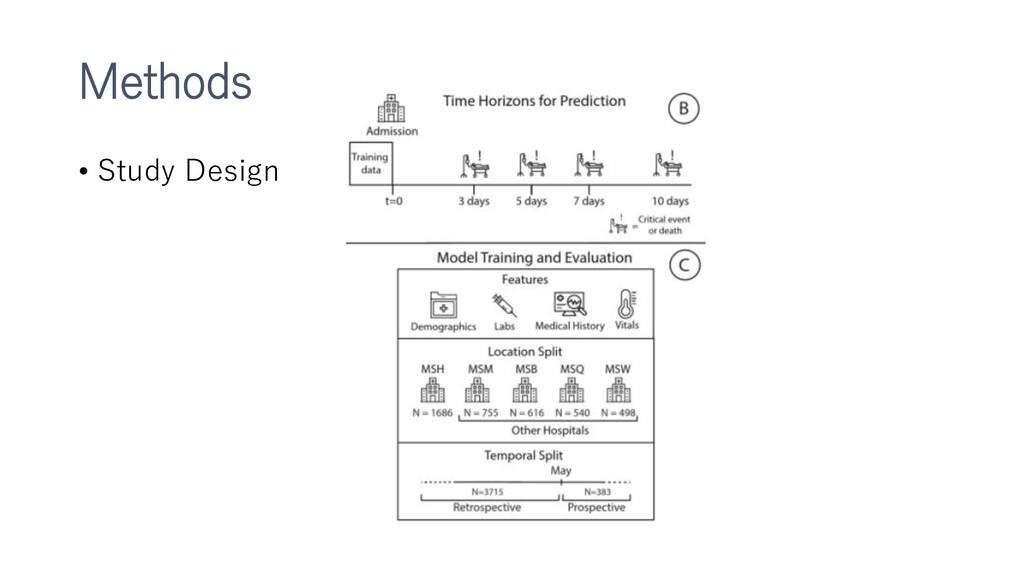
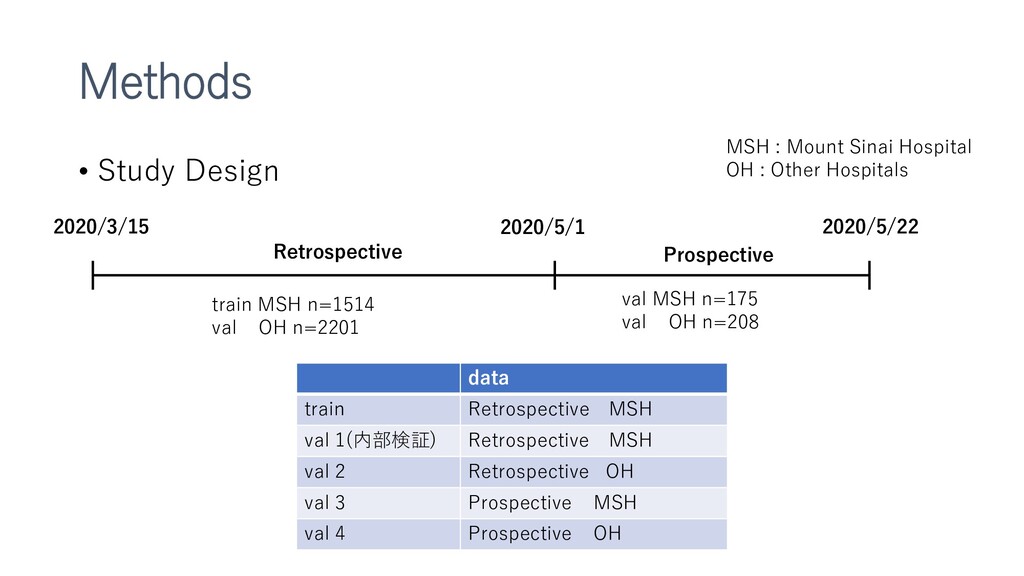
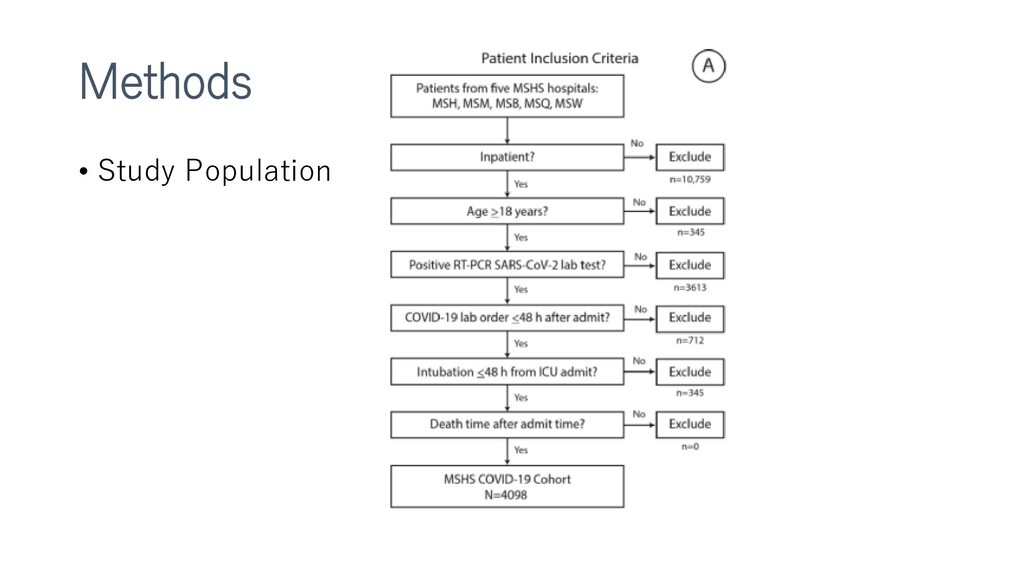
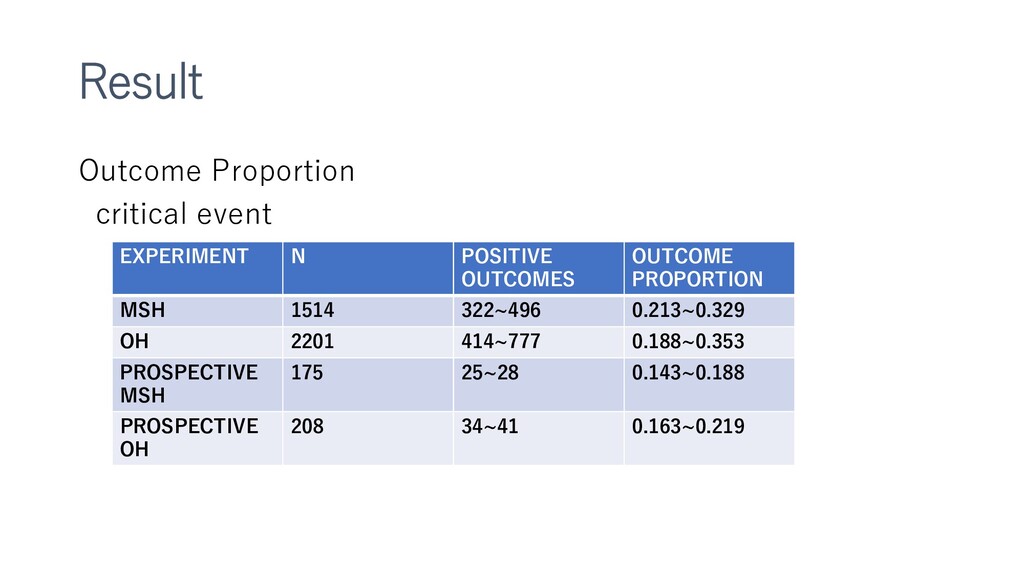
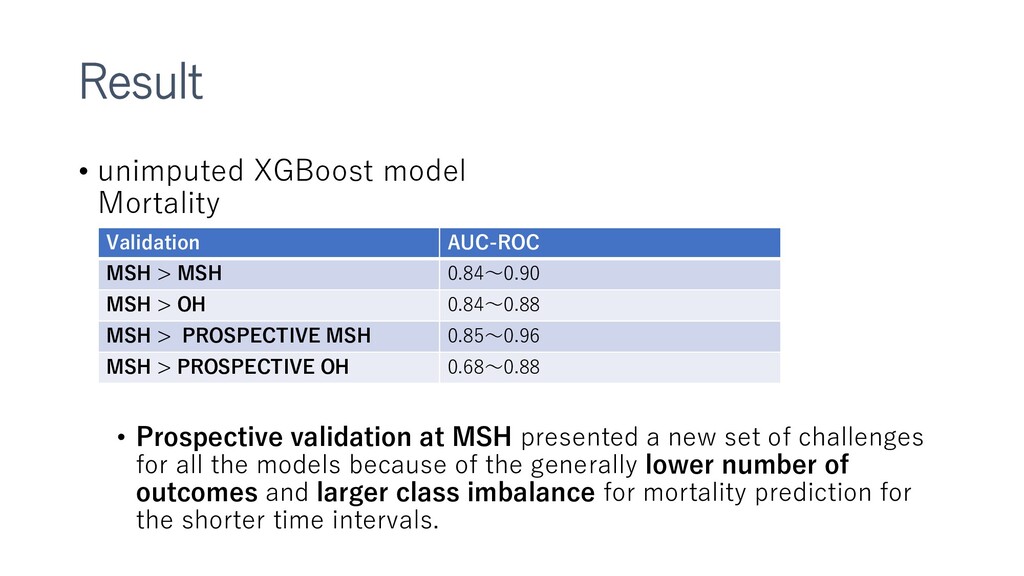
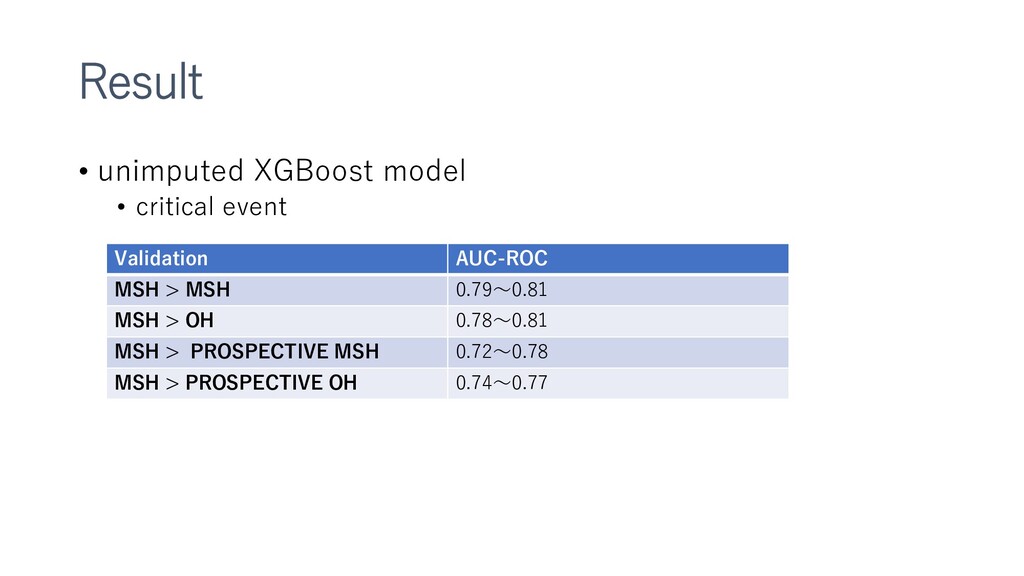
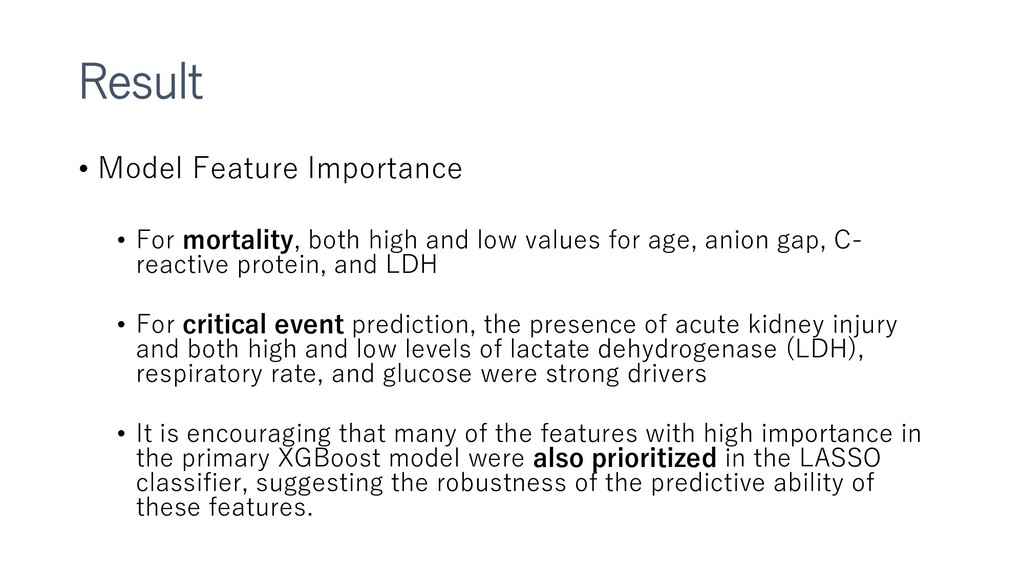
新型コロナウイルスによる死亡、重大イベントの予測をするXGboostモデルの作成など。多施設合同前向きで検証までやっているところがすごい。
各項目書き方が丁寧で、読んでいて非常に勉強になりました。
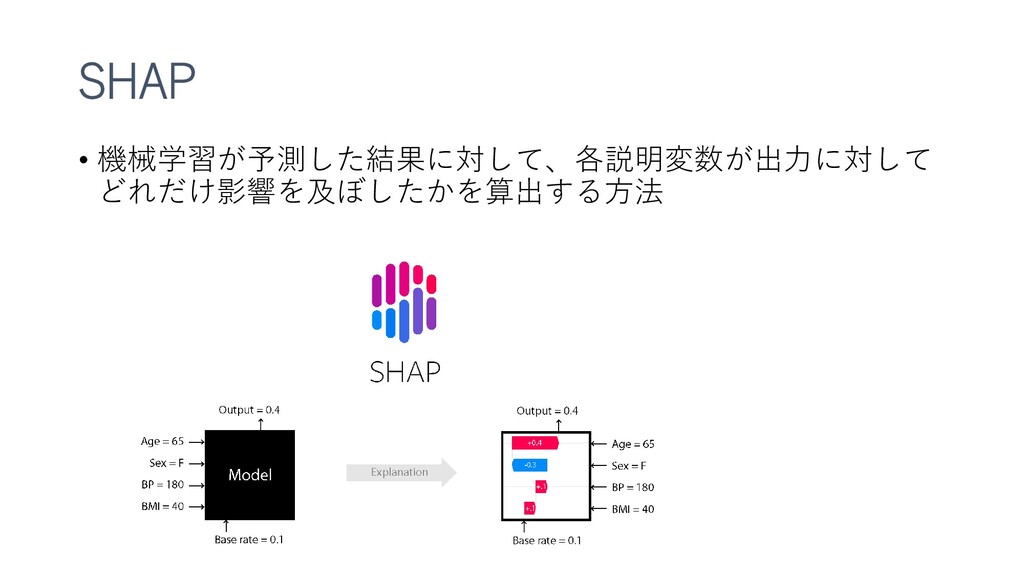
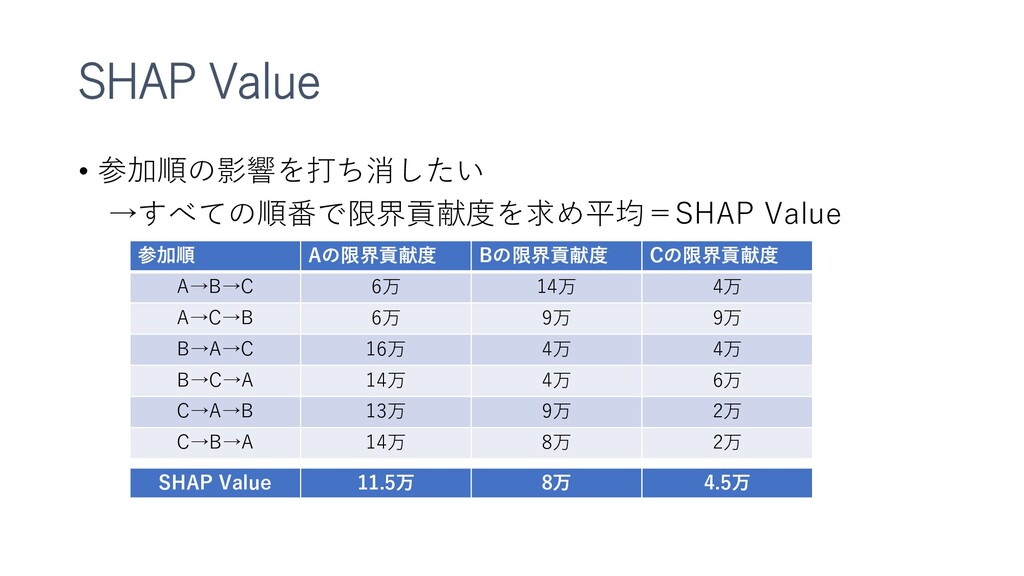
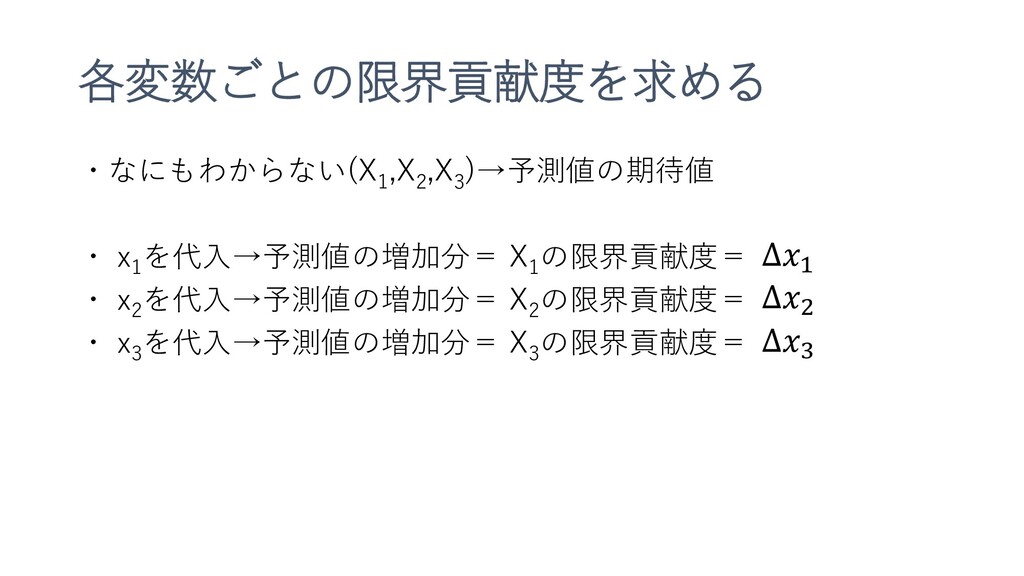
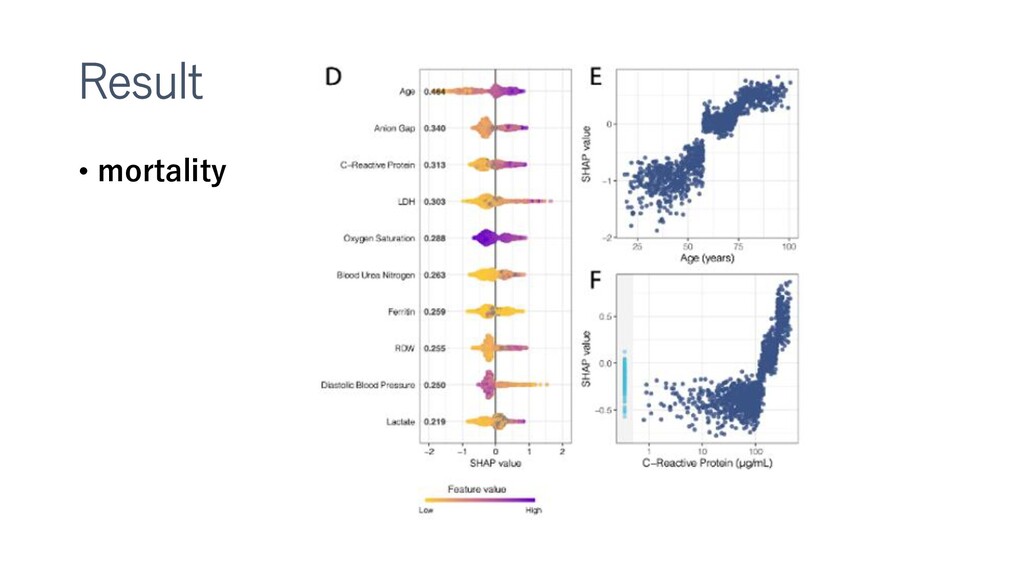
特徴重要度を得るSHAPについても紹介してみました。(複数記事のまとめなおしです)
Machine Learning to Predict Mortality and Critical Events in a Cohort of Patients With COVID-19 in New York City: Model Development and Validation
Published on 06.11.20
doi:10.2196/24018
Vaid A, Somani S, Russak AJ, De Freitas JK, Chaudhry FF, Paranjpe I, Johnson KW, Lee SJ, Miotto R, Richter F, Zhao S, Beckmann ND, Naik N, Kia A, Timsina P, Lala A, Paranjpe M, Golden E, Danieletto M, Singh M, Meyer D, O'Reilly PF, Huckins L, Kovatch P, Finkelstein J, Freeman RM, Argulian E, Kasarskis A, Percha B, Aberg JA, Bagiella E, Horowitz CR, Murphy B, Nestler EJ, Schadt EE, Cho JH, Cordon-Cardo C, Fuster V, Charney DS, Reich DL, Bottinger EP, Levin MA, Narula J, Fayad ZA, Just AC, Charney AW, Nadkarni GN, Glicksberg BS
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
![各変数ごとのSHAP Valueを求める 𝐸[𝑓 𝑥1 , 𝑥2 , 𝑋3 ] 𝐸[𝑓](https://files.speakerdeck.com/presentations/00b78740e94b4047925521cd2933334d/slide_33.jpg){kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}