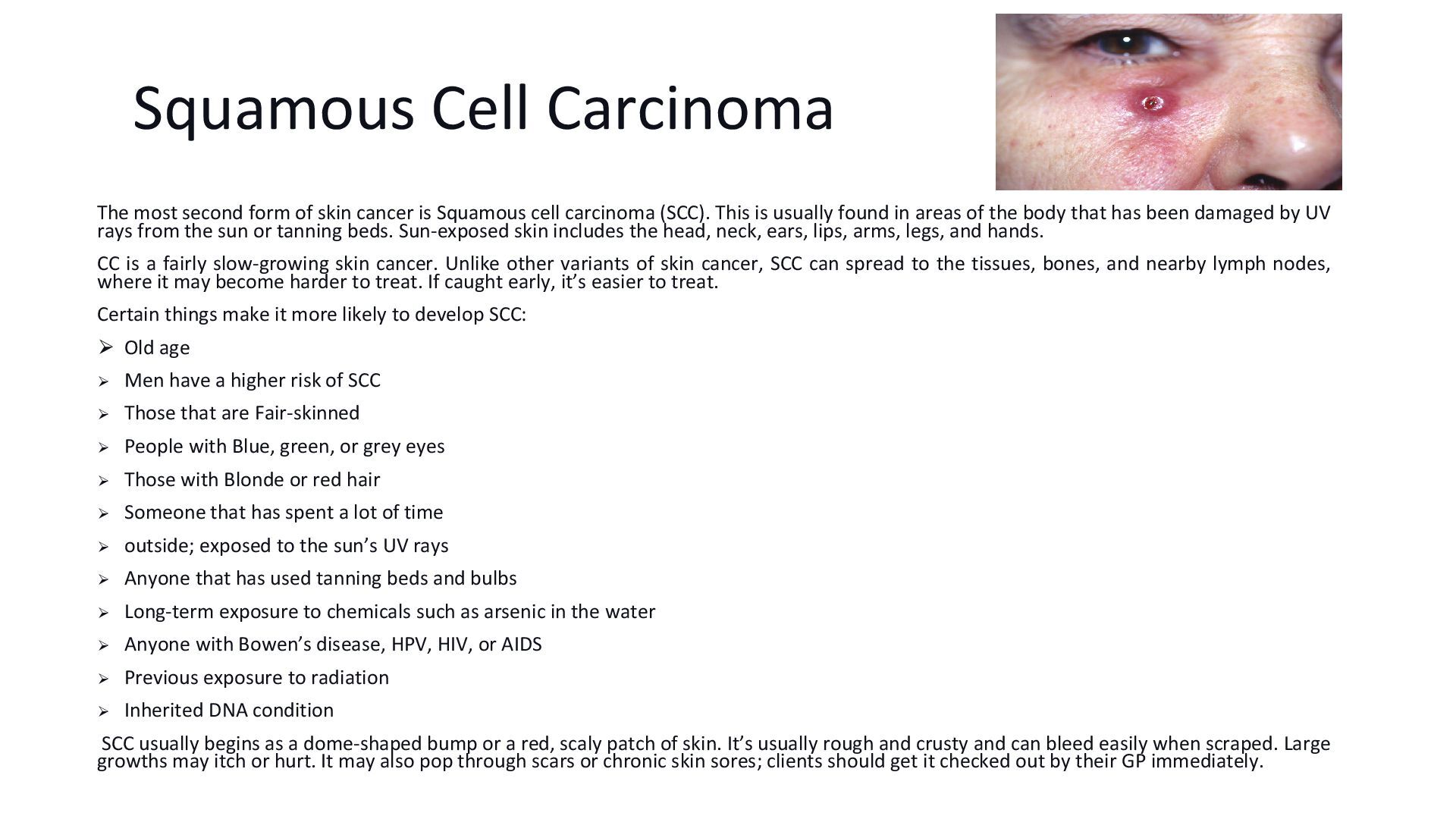
is Squamous cell carcinoma (SCC). This is usually found in areas of the body that has been damaged by UV rays from the sun or tanning beds. Sun-exposed skin includes the head, neck, ears, lips, arms, legs, and hands. CC is a fairly slow-growing skin cancer. Unlike other variants of skin cancer, SCC can spread to the tissues, bones, and nearby lymph nodes, where it may become harder to treat. If caught early, it’s easier to treat. Certain things make it more likely to develop SCC: ⮚ Old age ⮚ Men have a higher risk of SCC ⮚ Those that are Fair-skinned ⮚ People with Blue, green, or grey eyes ⮚ Those with Blonde or red hair ⮚ Someone that has spent a lot of time ⮚ outside; exposed to the sun’s UV rays ⮚ Anyone that has used tanning beds and bulbs ⮚ Long-term exposure to chemicals such as arsenic in the water ⮚ Anyone with Bowen’s disease, HPV, HIV, or AIDS ⮚ Previous exposure to radiation ⮚ Inherited DNA condition SCC usually begins as a dome-shaped bump or a red, scaly patch of skin. It’s usually rough and crusty and can bleed easily when scraped. Large growths may itch or hurt. It may also pop through scars or chronic skin sores; clients should get it checked out by their GP immediately.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}