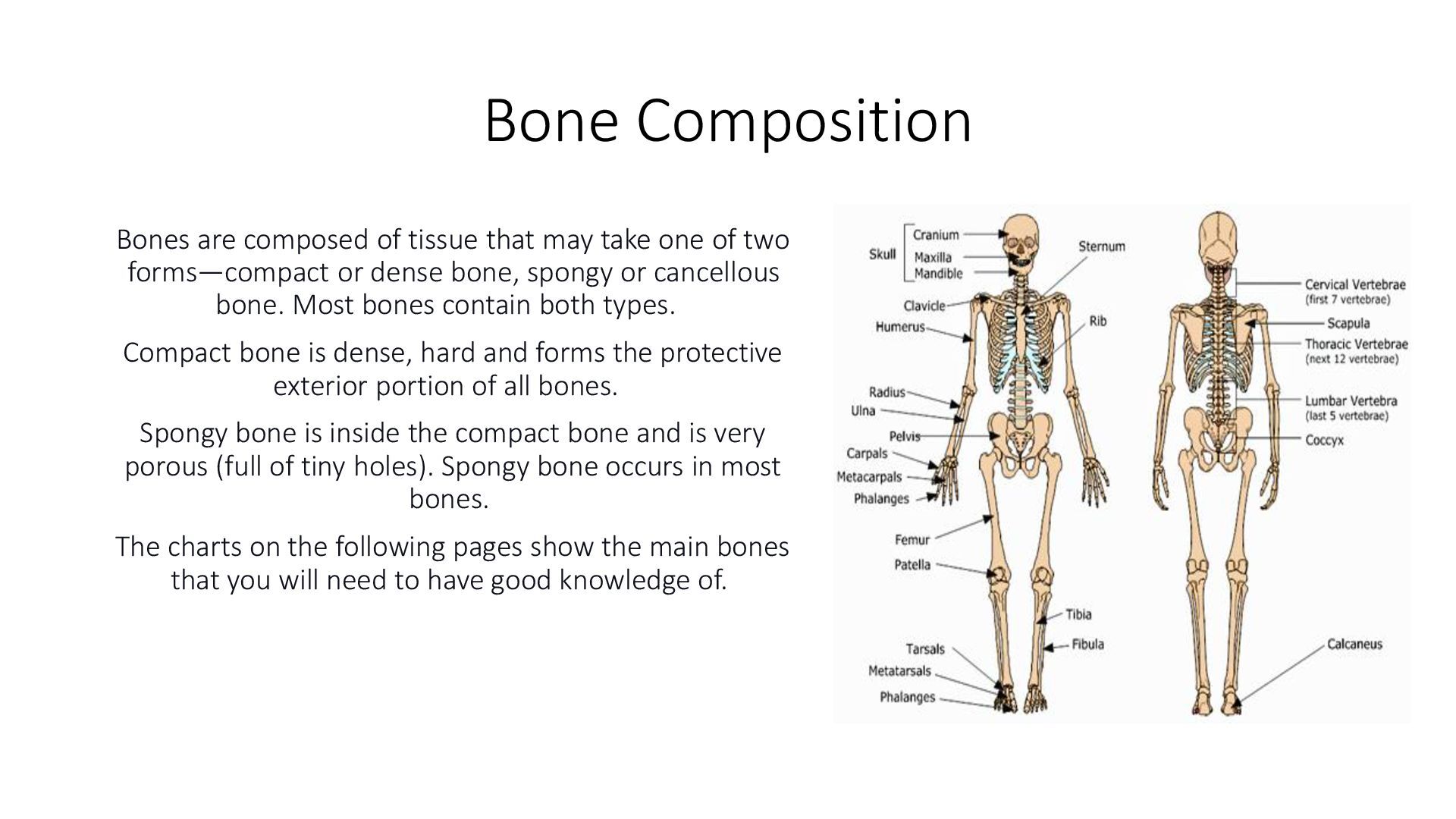
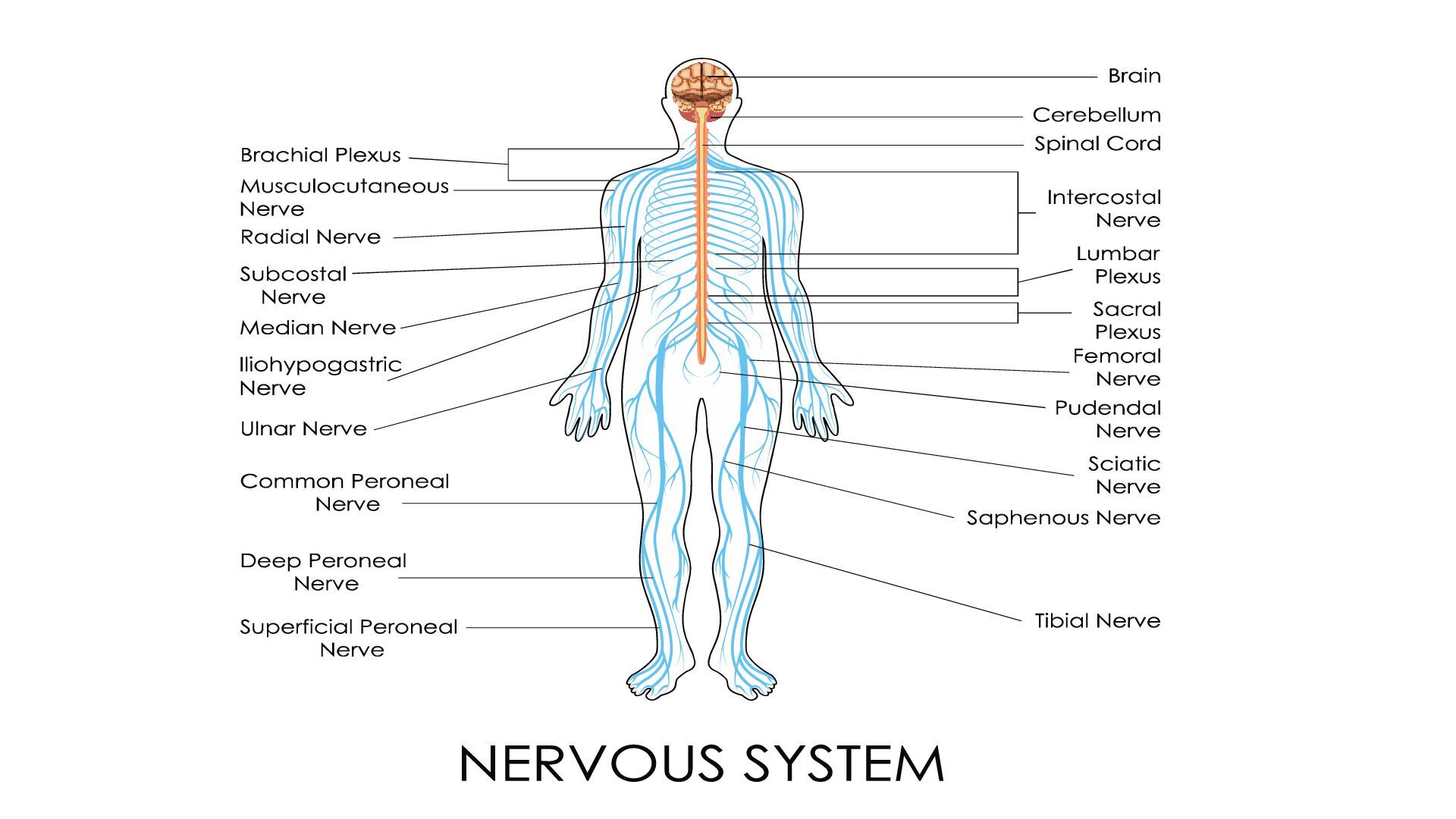
human body, most of which are in the brain. The nervous system can be thought of as two systems: The central nervous system (CNS) is made up of the brain and spinal cord, and the peripheral nervous system (PNS) is everything outside of the brain and spinal cord. Sensory neurons transmit nerve impulses to the spinal cord or the brain from muscle tissues. Motor neurons transmit impulses to muscles from the spinal cord or the brain. Both the brain and the spinal cord are covered by protective membranes (meninges). Between these protective membrane layers are spaces filled with cerebrospinal fluid (CSF) that provides a cushion for the brain and the spinal cord. Furthermore, the brain and spinal cord are protected by the skull and vertebral column, respectively. The bony segments of the vertebral canal are divided into regions (cervical, thoracic, and lumbar vertebrae). There are seven cervical vertebrae (C1- C7) that extend from the head to the thorax, 12 thoracic vertebrae (T1 T12) that extend from the chest to the back, and five lumbar vertebrae (L1-L5) that extend to the lower back. At the lower end of the vertebral column, the sacrum (S1-S5) and coccyx are fused elements of the sacral and coccygeal vertebrae. The brain, along with the cranial nerves, functions in all mental processes and many essential motor, sensory, and visceral responses. The spinal cord and the spinal nerves control sensory (touch), motor (voluntary movement), and reflex (knee-jerk) functions. Reflexes are responses to stimuli that do not require communication with the brain. A simple reflex, such as moving a finger from something hot, occurs even before the brain realises the pain. Specific cranial and spinal nerves control all complex or simple action processes in the body. There are 31 pairs of spinal nerves (nerves that branch off the spinal cord), each of which is identified by its location to the nearest vertebrae. Nerves that branch from the spinal cord (C5 through Tl) and extend into the arm region (the brachial plexus) are the axillary, radial, musculocutaneous, median, and ulnar nerves. These nerves control all muscle movement of the shoulder, arm, and hand and also control sensations of the skin of the entire shoulder, arm, and hand. In summary, the nervous system is the primary communication and regulatory system in the body. The autonomic nervous system entails the functions that work without voluntary control of an individual, such as heartbeat, rate of breathing, tear and saliva production, and bladder constrictions.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}