a patient with an incidental finding of bradycardia with a background of AN. It was apparent from a brief dip into the literature that this is a "relatively common" finding in this demographic. I endeavored to perform a quick literature review to determine the prevalence of ECG manifestations in AN.
ST-segment elevation, T-wave flattening, low voltage and a right-ward cardiac axis. These are clinically insignificant." "QTc prolongation however, may indicate risk of arrhythmia and sudden cardiac death." But I wanted to know more... Scratching the surface;
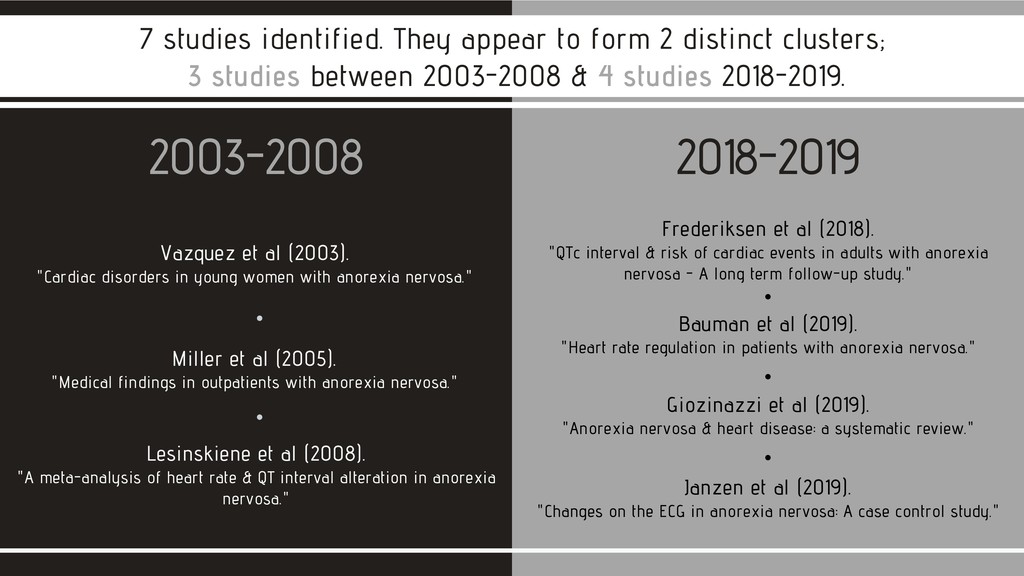
anorexia nervosa." 2003-2008 2018-2019 7 studies identified. They appear to form 2 distinct clusters; 3 studies between 2003-2008 & 4 studies 2018-2019. Miller et al (2005). "Medical findings in outpatients with anorexia nervosa." Lesinskiene et al (2008). "A meta-analysis of heart rate & QT interval alteration in anorexia nervosa." Bauman et al (2019). "Heart rate regulation in patients with anorexia nervosa." Frederiksen et al (2018). "QTc interval & risk of cardiac events in adults with anorexia nervosa - A long term follow-up study." Janzen et al (2019). "Changes on the ECG in anorexia nervosa: A case control study." Giozinazzi et al (2019). "Anorexia nervosa & heart disease: a systematic review."
patients with AN. LV mass was significantly lower in patients with AN. 'Significant relationship' between body mass index (BMI) and lower heart rate (HR), as well as between BMI and QTc prolongation. Vazquez et al (2003); Study population was only 30 patients, all female, aged 12-18.5 years. Care should be taken before assuming that these findings apply to the wider population - particularly to those over 18 and to males. As the study was very small and based at a single center, the overall conclusions may be considered less significant/robust. Conclusions; Noteworthy;
19.7% of patients had hyponatraemia Miller et al (2005); Study population was 214 patients, all female and all "college-aged". As with the previous study, care should be taken before assuming that these findings apply to the wider population - particularly to those over 21 and to males. This study was better populated, but still relatively small. Conclusions; Noteworthy; The probability of bradycardia could be predicted by the degree of malnutrition.
HR and BMI decreases as the disease continues. QTc was in range in AN, but still significantly longer than in controls. MEDLINE search between 1994-2005 for studies including anorexia + measurement of HR + measurement of QTc interval. 10 studies found.
mean QTc interval or risk of QTc prolongation between AN patients and healthy controls. AN patients had a significantly increased risk of aborted cardiac arrest, cardiac arrest - unrelated to the baseline QTc interval. All cause mortality increased in AN. Study population was 430 patients, all female. Once again, care should be taken before assuming that these findings apply to males. Additionally, whilst this was a larger study, it was still relatively small. Noteworthy;
HR variability showed signs of saturation in patients with AN. The are neural and non-neural mechanisms responsible for HR variability and bradycardia in AN. HCN4 down-regulation may go some way to explain the impact of AN on HR. (HCN4 is a potassium/sodium hyperpolarisation- activated channel predominantly expressed in the pacemaker region of the mammalian heart). Study population was 20 patients, male AND female, aged between 12 and 16. Once again, care should be taken before assuming that these findings are more widely applicable. Additionally, this was also a very small, single-center study. Noteworthy;
and QTc prolongation. Also found was reduced cardiac mass with smaller volumes and decreased cardiac output. Mitral valve prolapse and pericardial effusion may occur due to protein deficiency and reduced thyroid hormone. No conclusive evidence that AN is atherogenic. In refeeding syndrome there was found to be an increased risk of life-threatening cardiac complications. Large, systematic literature review. Noteworthy;
AN. QT interval longer in AN, but similar to controls when corrected for HR (QTc). Prevalence of T-wave flattening and T-wave inversion were similar to controls. Another very small, single-center study. Noteworthy;
prolapse & pericardial effusion have been observed when larger populations studied. 4 Bradycardia is a common finding in anorexia nervosa. 2 All-cause mortality increased in AN, including from cardiac arrest. 3 1 There is a clear link between AN & prolonged QT interval. Link is less strong when corrected for HR (QTc).
attempting to conserve energy by reducing cardiac output. Electrolyte loss, drugs w/ adverse cardiovascular effects, reduced glycogen content in heart cells, myofibrillar atrophy, interstitial oedema, mitochondiral tumefaction & activation of calcium dependent proteinaises. Hypotheses that have been suggested; Others.. Down-regulation of HCN4; (A potassium/sodium hyperpolarisation-activated channel predominantly expressed in the pacemaker region of the mammalian heart).
in LV mass. Alteration of ion channels, increased fibrous tissue, myocardial degeneration, myocytolysis, mononuclear infiltrate, fat infiltrate and substitution of muscle tissue for collagen. Hypotheses that have been suggested; Others.. Histologic changes & alterations of the cardiac muscle fibres.
must be careful not to dismiss them without due consideration. 2 OP monitoring - in the form of 24hr holter, or transthoracic echocardiogram for example - and follow-up may be clinically indicated. 3 1 QT prolongation may need to be mitigated by elimination/avoidance of drugs that exacerbate this (eg some antidepressants, antiarrhythmics, antihistamines, antimicrobials). A full list can be found here; www.listsandlaughter.com/2016/08/04/drugs-to-avoid/
with anorexia nervosa. Available at https://doi.org/10.31234/osf.io/qpgz4. Janzen et al (2019) Changes on the ECG in anorexia nervosa: A case control study. Journal of Electrocardiology. Vol 56, Sept-Oct 2019, pg64-69. Frederiksen, et al (2018) QTc interval and risk of cardiac events in adults with anorexia nervosa - A long term follow-up study. Circulation: Arrhythmia and electrophysiology. 2018; 11. Giovinazzo et al (2019) Anorexia nervosa and heart disease: a systematic review. Eating and weight disorders - Studies on anorexia, bulimia and obesity. April 19, vol 24, iss 2, pp 199-207. Lesinskiene, et al (2008) A meta-analysis of heart rate and QT interval alteration in anorexia nervosa. World Journal of Bilogical Psychiatry. 2008 9(2):86-91. Miller et al (2005) Medical findings in outpaitnets with anorexia nervosa. Archive Internal Medicine. 2005; 165(5): 561-6. Vazquez et al (2003) Cardiac disorders in young women with anorexia nervosa. Revista espanola de cardiologia. 2003; 56(7):669- 73. REFERENCES;
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}