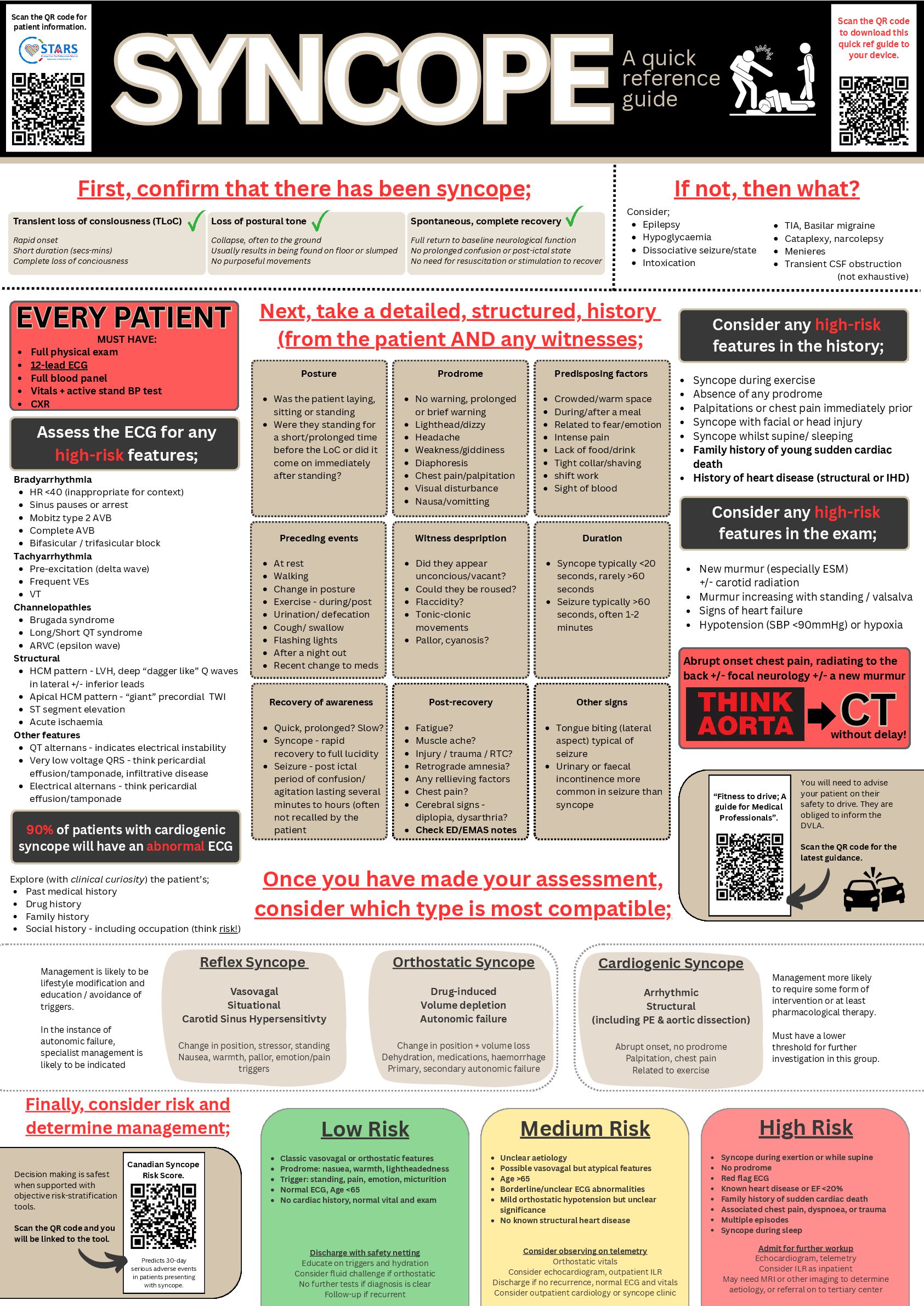
complete recovery SYNCOPE SYNCOPEA quick reference guide Canadian Syncope Risk Score. Predicts 30-day serious adverse events in patients presenting with syncope. Decision making is safest when supported with objective risk-stratification tools. Scan the QR code and you will be linked to the tool. You will need to advise your patient on their safety to drive. They are obliged to inform the DVLA. Scan the QR code for the latest guidance. “Fitness to drive; A guide for Medical Professionals”. First, confirm that there has been syncope; Rapid onset Short duration (secs-mins) Complete loss of conciousness Collapse, often to the ground Usually results in being found on floor or slumped No purposeful movements Full return to baseline neurological function No prolonged confusion or post-ictal state No need for resuscitation or stimulation to recover If not, then what? Consider; Epilepsy Hypoglycaemia Dissociative seizure/state Intoxication TIA, Basilar migraine Cataplexy, narcolepsy Menieres Transient CSF obstruction (not exhaustive) Assess the ECG for any high-risk features; Next, take a detailed, structured, history (from the patient AND any witnesses; Consider any high-risk features in the history; Bradyarrhythmia HR <40 (inappropriate for context) Sinus pauses or arrest Mobitz type 2 AVB Complete AVB Bifasicular / trifasicular block Tachyarrhythmia Pre-excitation (delta wave) Frequent VEs VT Channelopathies Brugada syndrome Long/Short QT syndrome ARVC (epsilon wave) Structural HCM pattern - LVH, deep “dagger like” Q waves in lateral +/- inferior leads Apical HCM pattern - “giant” precordial TWI ST segment elevation Acute ischaemia Other features QT alternans - indicates electrical instability Very low voltage QRS - think pericardial effusion/tamponade, infiltrative disease Electrical alternans - think pericardial effusion/tamponade 90% of patients with cardiogenic syncope will have an abnormal ECG Abrupt onset chest pain, radiating to the back +/- focal neurology +/- a new murmur Consider any high-risk features in the exam; New murmur (especially ESM) +/- carotid radiation Murmur increasing with standing / valsalva Signs of heart failure Hypotension (SBP <90mmHg) or hypoxia CT CT without delay! Syncope during exercise Absence of any prodrome Palpitations or chest pain immediately prior Syncope with facial or head injury Syncope whilst supine/ sleeping Family history of young sudden cardiac death History of heart disease (structural or IHD) Posture Was the patient laying, sitting or standing Were they standing for a short/prolonged time before the LoC or did it come on immediately after standing? Prodrome No warning, prolonged or brief warning Lighthead/dizzy Headache Weakness/giddiness Diaphoresis Chest pain/palpitation Visual disturbance Nausa/vomitting Predisposing factors Crowded/warm space During/after a meal Related to fear/emotion Intense pain Lack of food/drink Tight collar/shaving shift work Sight of blood Preceding events At rest Walking Change in posture Exercise - during/post Urination/ defecation Cough/ swallow Flashing lights After a night out Recent change to meds Witness despription Did they appear unconcious/vacant? Could they be roused? Flaccidity? Tonic-clonic movements Pallor, cyanosis? Duration Syncope typically <20 seconds, rarely >60 seconds Seizure typically >60 seconds, often 1-2 minutes Recovery of awareness Quick, prolonged? Slow? Syncope - rapid recovery to full lucidity Seizure - post ictal period of confusion/ agitation lasting several minutes to hours (often not recalled by the patient Post-recovery Fatigue? Muscle ache? Injury / trauma / RTC? Retrograde amnesia? Any rellieving factors Chest pain? Cerebral signs - diplopia, dysarthria? Check ED/EMAS notes Other signs Tongue biting (lateral aspect) typical of seizure Urinary or faecal incontinence more common in seizure than syncope Once you have made your assessment, consider which type is most compatible; Reflex Syncope Vasovagal Situational Carotid Sinus Hypersensitivty Change in position, stressor, standing Nausea, warmth, pallor, emotion/pain triggers Orthostatic Syncope Drug-induced Volume depletion Autonomic failure Change in position + volume loss Dehydration, medications, haemorrhage Primary, secondary autonomic failure Cardiogenic Syncope Arrhythmic Structural (including PE & aortic dissection) Abrupt onset, no prodrome Palpitation, chest pain Related to exercise Explore (with clinical curiosity) the patient’s; Past medical history Drug history Family history Social history - including occupation (think risk!) Management is likely to be lifestyle modification and education / avoidance of triggers. In the instance of autonomic failure, specialist management is likely to be indicated Management more likely to require some form of intervention or at least pharmacological therapy. Must have a lower threshold for further investigation in this group. Scan the QR code to download this quick ref guide to your device. Low Risk Classic vasovagal or orthostatic features Prodrome: nasuea, warmth, lightheadedness Trigger: standing, pain, emotion, micturition Normal ECG, Age <65 No cardiac history, normal vital and exam Discharge with safety netting Educate on triggers and hydration Consider fluid challenge if orthostatic No further tests if diagnosis is clear Follow-up if recurrent Medium Risk Unclear aetiology Possible vasovagal but atypical features Age >65 Borderline/unclear ECG abnormalities Mild orthostatic hypotension but unclear significance No known structural heart disease Consider observing on telemetry Orthostatic vitals Consider echocardiogram, outpatient ILR Discharge if no recurrence, normal ECG and vitals Consider outpatient cardiology or syncope clinic High Risk Syncope during exertion or while supine No prodrome Red flag ECG Known heart disease or EF <20% Family history of sudden cardiac death Associated chest pain, dyspnoea, or trauma Multiple episodes Syncope during sleep Admit for further workup Echocardiogram, telemetry Consider ILR as inpatient May need MRI or other imaging to determine aetiology, or referral on to tertiary center Finally, consider risk and determine management; MUST HAVE: Full physical exam 12-lead ECG Full blood panel Vitals + active stand BP test CXR EVERY PATIENT EVERY PATIENT Scan the QR code for patient information.
{kind=link}