Care (since 1955) • Definitions & Decision Points • Best Practices post-1955 • Stratifying by Risk of Colectomy • Improving Your Practice with Outcome Data • A Pilot Trial • Where Can We Improve? • Future State
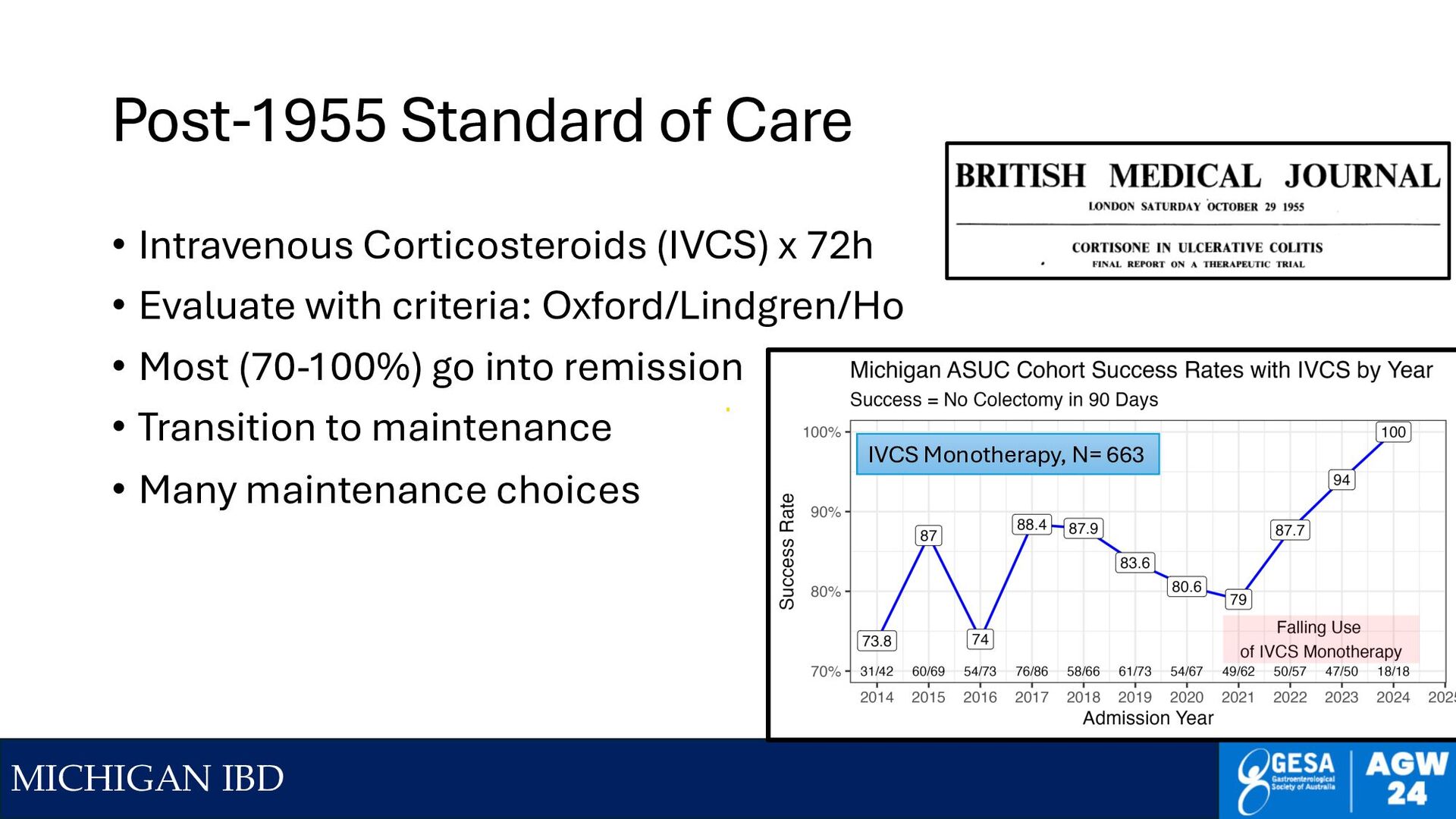
Corticosteroids (IVCS) x 72h • Evaluate with criteria: Oxford/Lindgren/Ho • Most (70-100%) go into remission • Transition to maintenance • Many maintenance choices IVCS Monotherapy, N= 663
Criteria for ASUC in 1955 (no one admitted on steroids) • >= 6 BM/day with visible blood AND 1 or more of • Anemia <= 10.5 g/L of Hgb • Fever > 100F/37.8C • Tachycardia > 90 BPM • ESR > 30 mm/hr • Alternate (lab) definition - classify by FCP • FCP > 782 ~ T&W severe UC • How many outpatients have Calpro >782? • Walking around (or running to toilet) with 1955 ASUC… 2024: My patient does not meet T&W criteria for ASUC - Unless I stop the 60 mg of daily prednisone Kedia, S, et al Dig Dis Sci 2018;63:2747-53
Abby is a 29 y/o F with pancolonic UC, never smoker • Initially on 5-ASA in Jan after prednisone taper, then urgency returned • April started on Aza 2.5 mg/kg, but HA and N/V – stopped after 4 weeks • Started IFX in July b/c flare – worked somewhat for first 3 doses • Admitted with 18 BM/day, blood in ~90%, temp 38.1, very thirsty • C diff negative by toxin, other infections ruled out by PCR • Has not eaten in 2d, because “it goes right through me” • Urgency time ~ 20 seconds • Hgb 7.9, ESR 46, CRP 124 mg/L, Alb 31 → 26 with fluids Risk Factors: CRP, ESR up Alb down Hgb down, fever, Prior Adv Rx
IVCS really still the best first line ASUC therapy? • They are fast & effective in ~ 70%+ • But have lots of side effects, and possibly cause long-term Rx resistance • And we have usually selected AGAINST some fast responders because we have already tried outpatient CS (prednisone) • Other options • Cyclosporine is pretty fast, lots of side effects, not maintenance • IFX is not that fast, leaks a lot, antibodies – kicks can down the road • JAKi are very fast, no leak, no antibodies – relatively few AEs vs CS, can be maintenance or can be a bridge
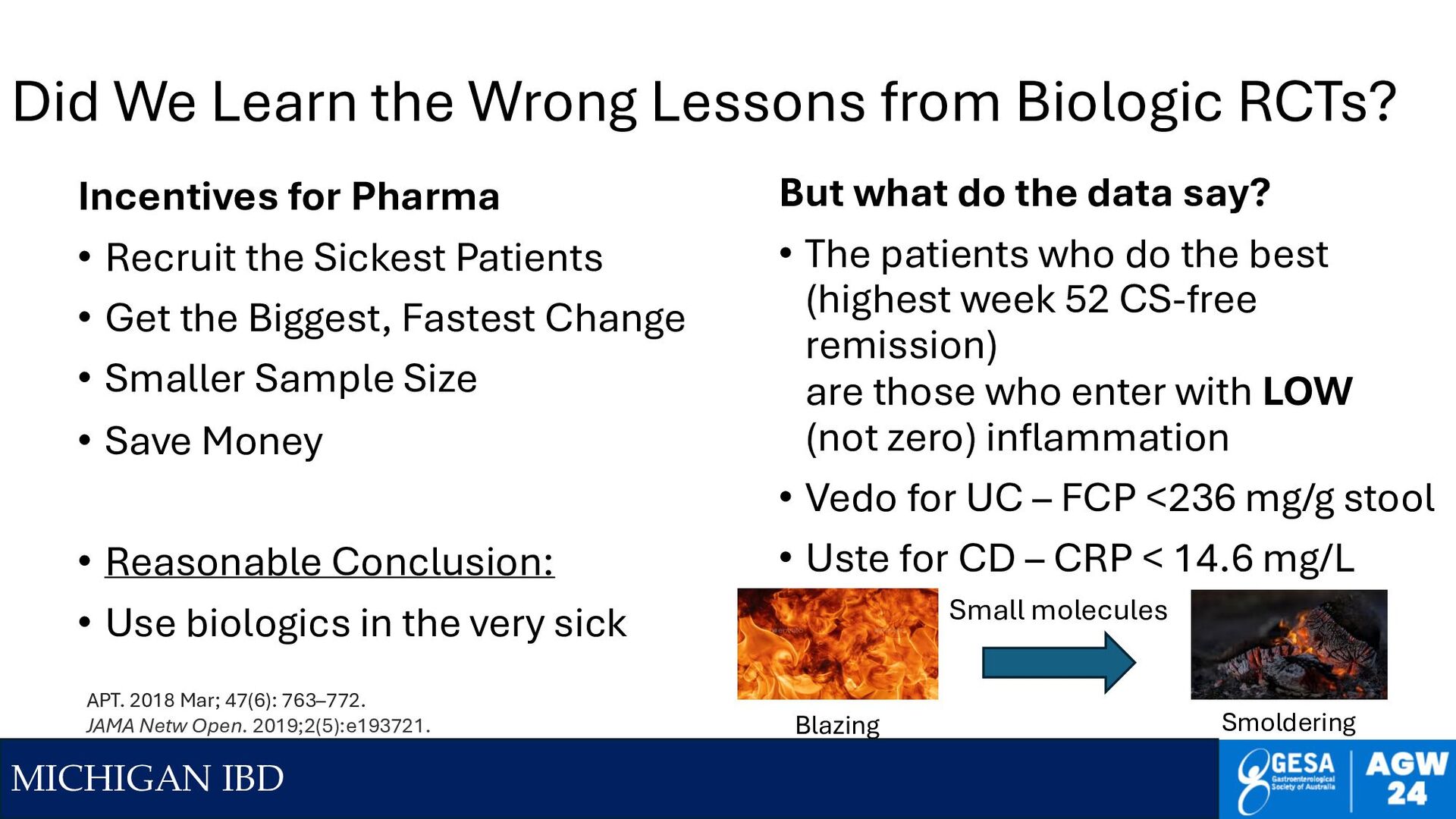
RCTs? Incentives for Pharma • Recruit the Sickest Patients • Get the Biggest, Fastest Change • Smaller Sample Size • Save Money • Reasonable Conclusion: • Use biologics in the very sick But what do the data say? • The patients who do the best (highest week 52 CS-free remission) are those who enter with LOW (not zero) inflammation • Vedo for UC – FCP <236 mg/g stool • Uste for CD – CRP < 14.6 mg/L APT. 2018 Mar; 47(6): 763–772. JAMA Netw Open. 2019;2(5):e193721. Small molecules Blazing Smoldering
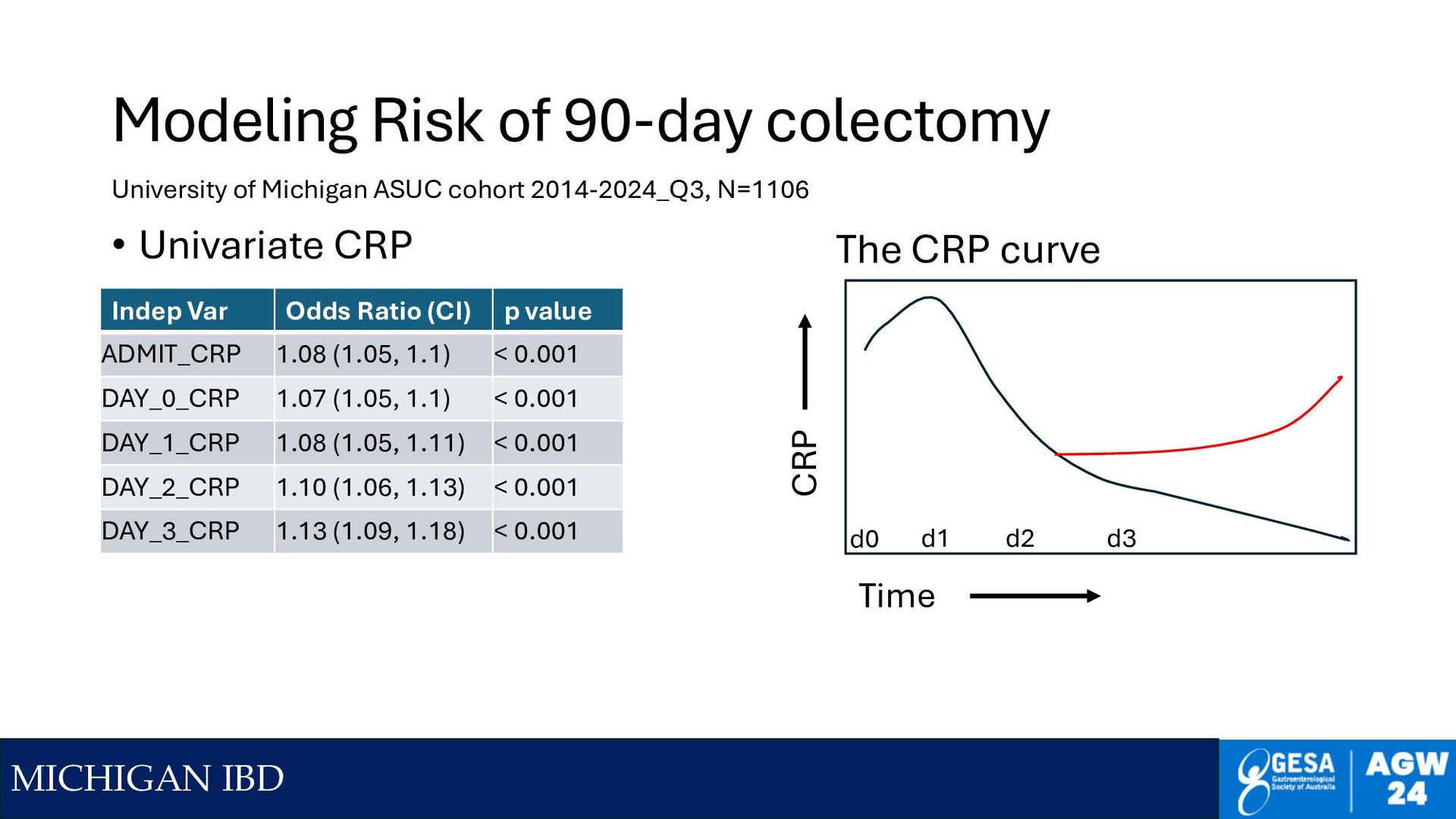
infections, perforation • Do early flexible sigmoidoscopy < 24h • Give lots of fluids early, be slow to feed, be very slow to TPN • Track CRP daily, FCP at discharge • Figure out noninvasive tracking – can’t scope daily, heal too slowly • Mucosal healing and FCP are relatively slow to normalize • Clinical improvement ≠ Out of the woods
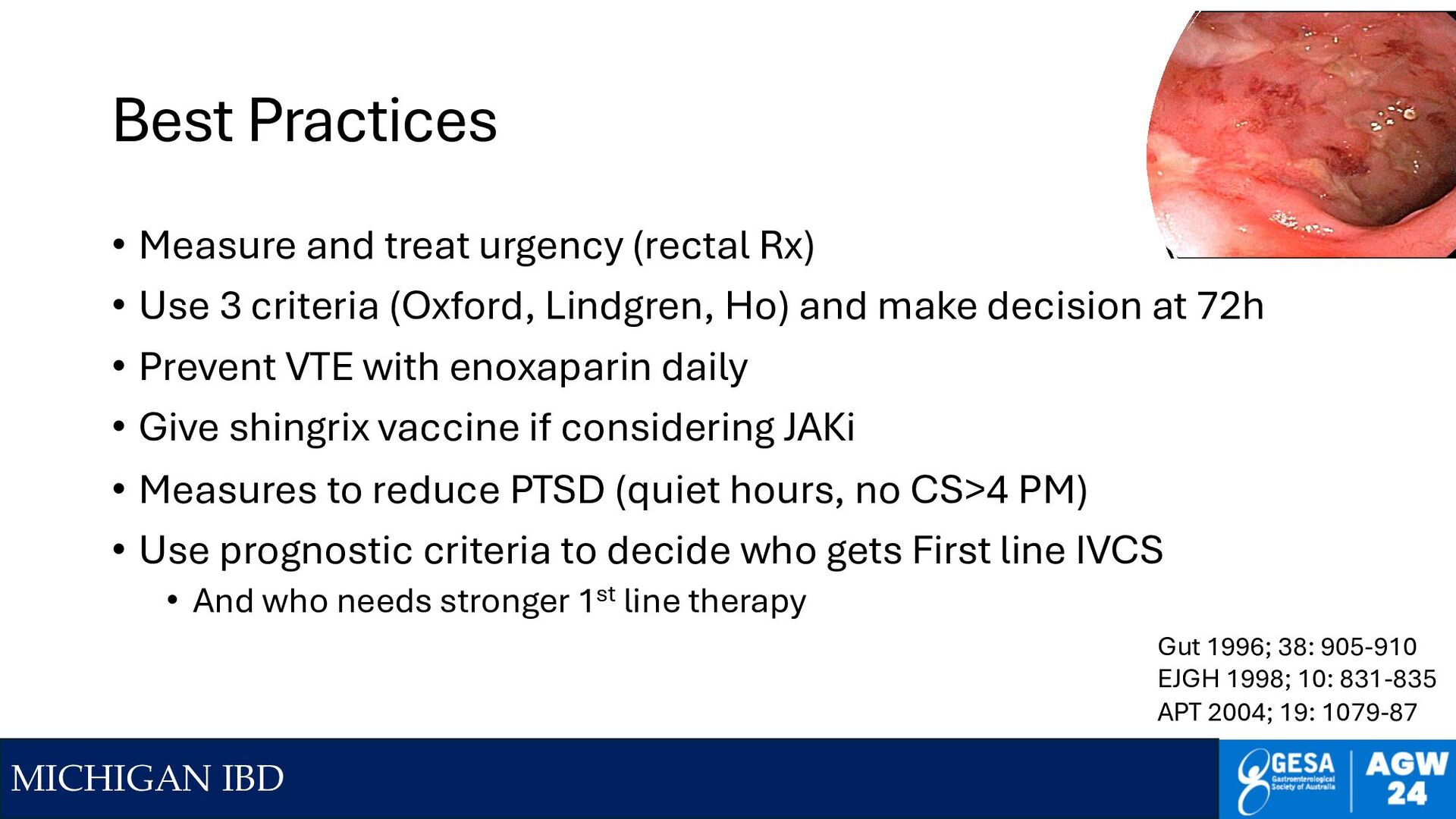
urgency (rectal Rx) • Use 3 criteria (Oxford, Lindgren, Ho) and make decision at 72h • Prevent VTE with enoxaparin daily • Give shingrix vaccine if considering JAKi • Measures to reduce PTSD (quiet hours, no CS>4 PM) • Use prognostic criteria to decide who gets First line IVCS • And who needs stronger 1st line therapy Gut 1996; 38: 905-910 EJGH 1998; 10: 831-835 APT 2004; 19: 1079-87
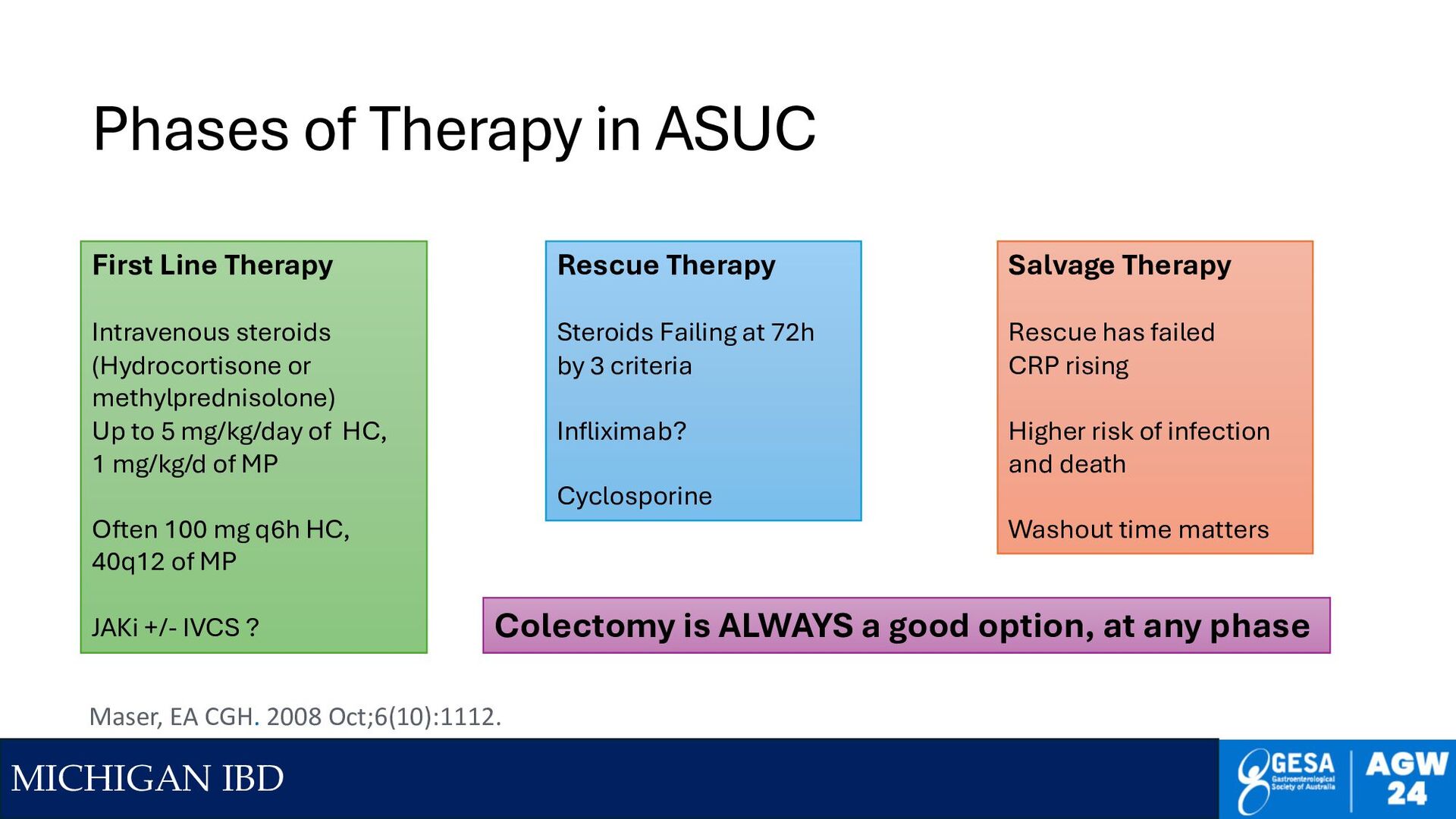
Line Therapy Intravenous steroids (Hydrocortisone or methylprednisolone) Up to 5 mg/kg/day of HC, 1 mg/kg/d of MP Often 100 mg q6h HC, 40q12 of MP JAKi +/- IVCS ? Rescue Therapy Steroids Failing at 72h by 3 criteria Infliximab? Cyclosporine Salvage Therapy Rescue has failed CRP rising Higher risk of infection and death Washout time matters Colectomy is ALWAYS a good option, at any phase Maser, EA CGH. 2008 Oct;6(10):1112.
in 1955? • RCTs in ASUC are hard • Not a lot of patients • ASUC T&W Criteria quite strict for 2024 • Patients anxious, not familiar with trials • Slow to recruit, patients reluctant to enroll • Physicians often reluctant to randomize • 2014: Evolve Therapies through QI approach • When we are confident, run RCTs to prove Rx works Uphill Climb to ASUC RCTs
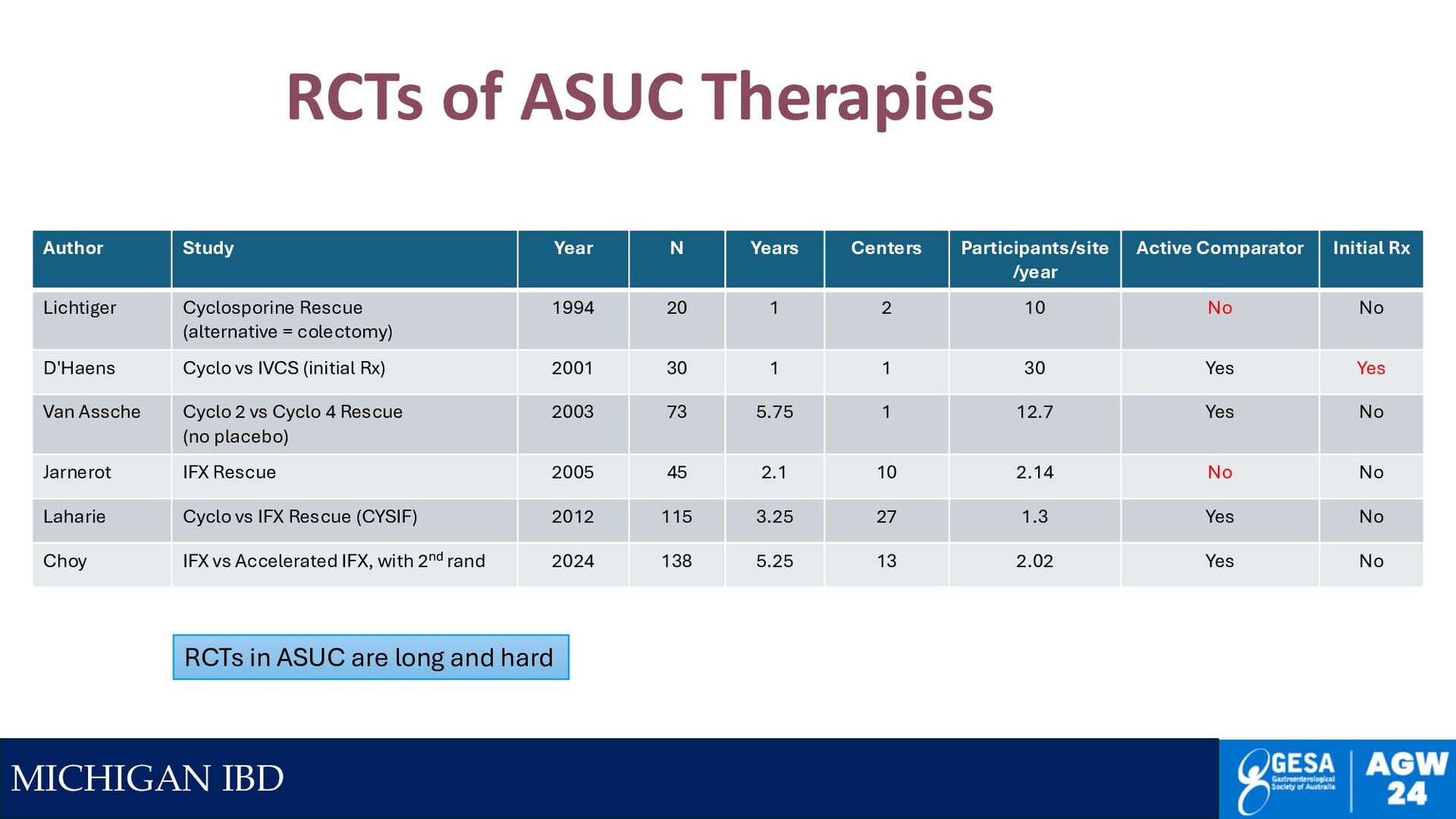
Active Comparator Initial Rx Lichtiger Cyclosporine Rescue (alternative = colectomy) 1994 20 1 2 10 No No D'Haens Cyclo vs IVCS (initial Rx) 2001 30 1 1 30 Yes Yes Van Assche Cyclo 2 vs Cyclo 4 Rescue (no placebo) 2003 73 5.75 1 12.7 Yes No Jarnerot IFX Rescue 2005 45 2.1 10 2.14 No No Laharie Cyclo vs IFX Rescue (CYSIF) 2012 115 3.25 27 1.3 Yes No Choy IFX vs Accelerated IFX, with 2nd rand 2024 138 5.25 13 2.02 Yes No RCTs in ASUC are long and hard RCTs of ASUC Therapies
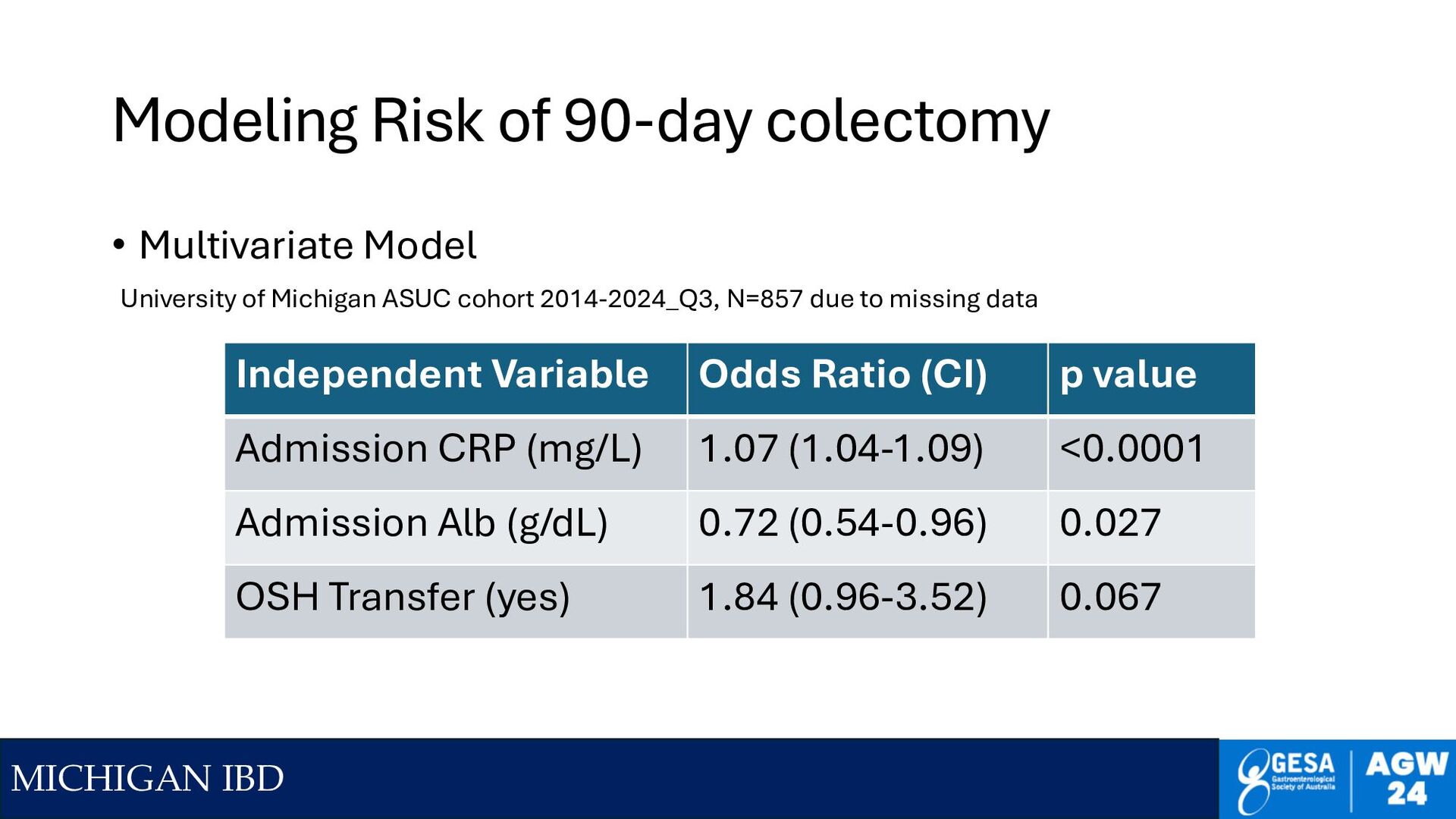
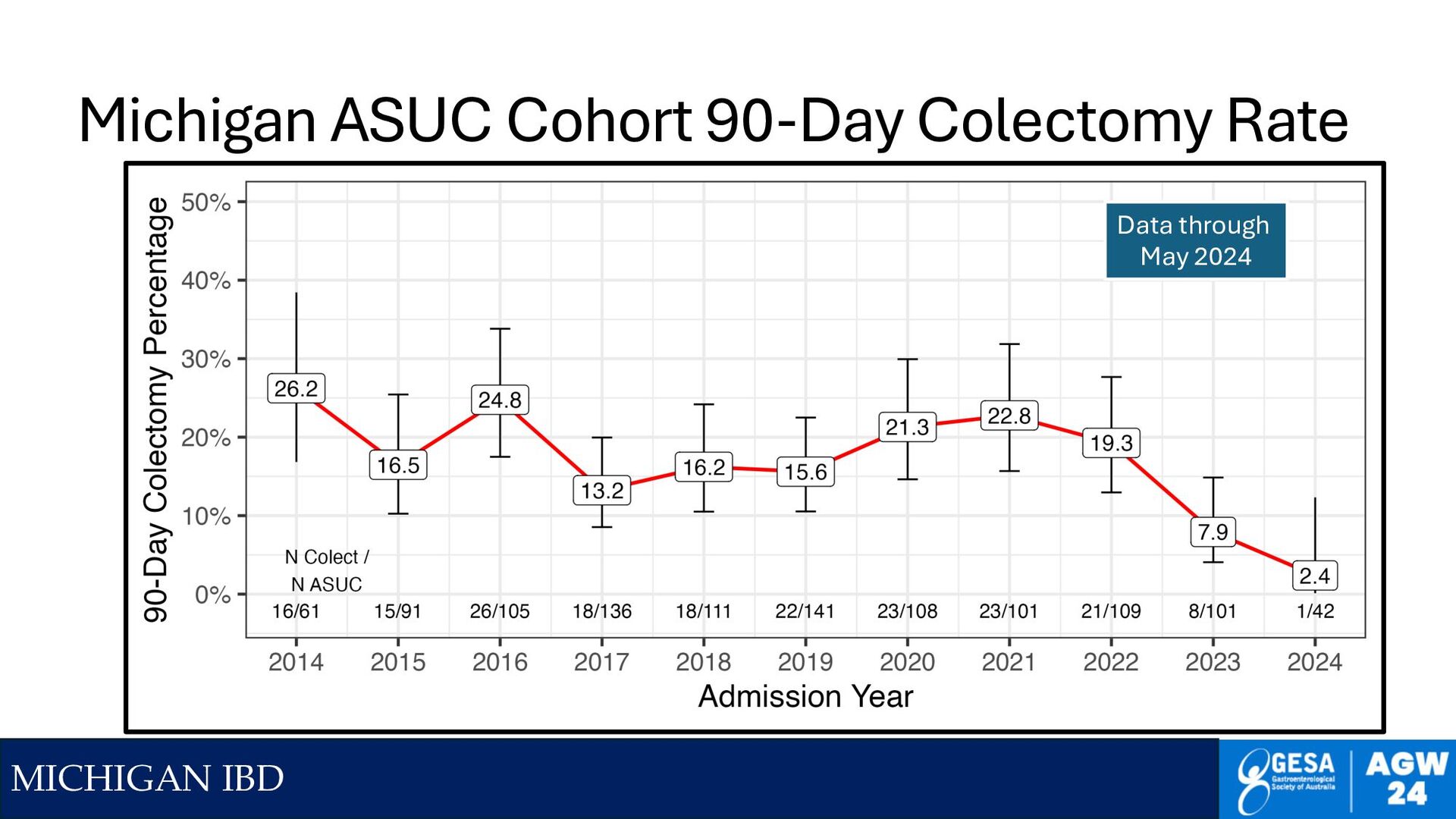
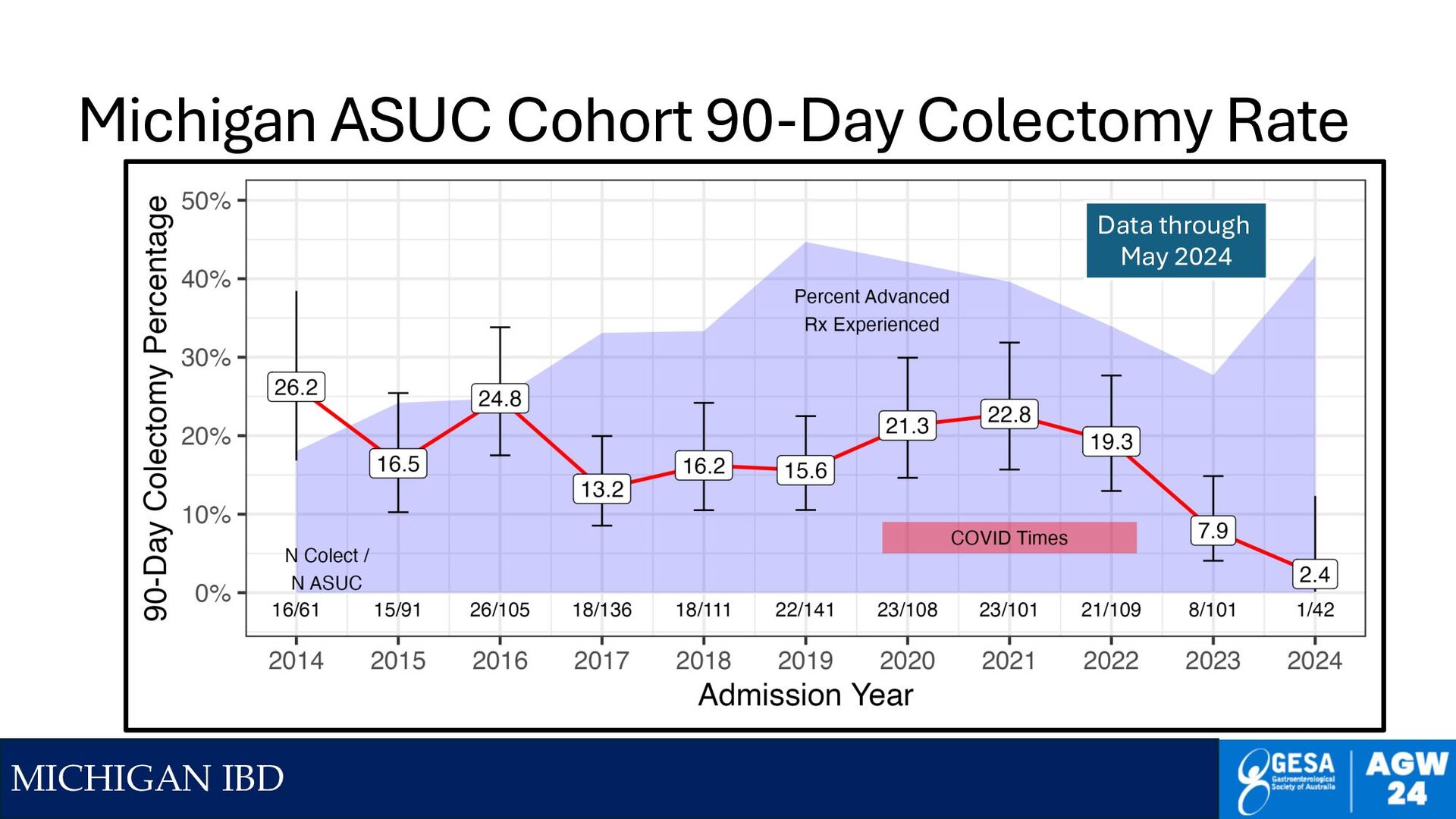
Multivariate Model Independent Variable Odds Ratio (CI) p value Admission CRP (mg/L) 1.07 (1.04-1.09) <0.0001 Admission Alb (g/dL) 0.72 (0.54-0.96) 0.027 OSH Transfer (yes) 1.84 (0.96-3.52) 0.067 University of Michigan ASUC cohort 2014-2024_Q3, N=857 due to missing data
Protocol • Standardize Therapy with a protocol • All components of care – control all the other variables • Get EVERYONE to compromise, agree to it • Require data, not vibes • Vibes = new questions to test • Make it public • Hold yourselves accountable – make it public • https://www.med.umich.edu/ibd/docs/severeucprotocol.pdf • Collect data on your outcomes • Try to improve, measure outcomes • If outcomes are not improving, try something else Plan Act Measure Change
by testing ‘accelerated’ infliximab • To overcome colonic leak • Rescue after 72h IVCS • Dosed at 10 mg/kg, repeat q72h (up to 3 doses) • Could get some patients out of the hospital • Many returned within 90 days for colectomy • Lots of failure between week 6 and week 14 • None of the patients with 3 doses avoided colectomy • Data were not superior to historical 1 dose IFX rescue • Slightly worse (30.3% vs 24.2%) Govani, SM, Higgins, Dig Dis Sci 2020;65:1800-1805.
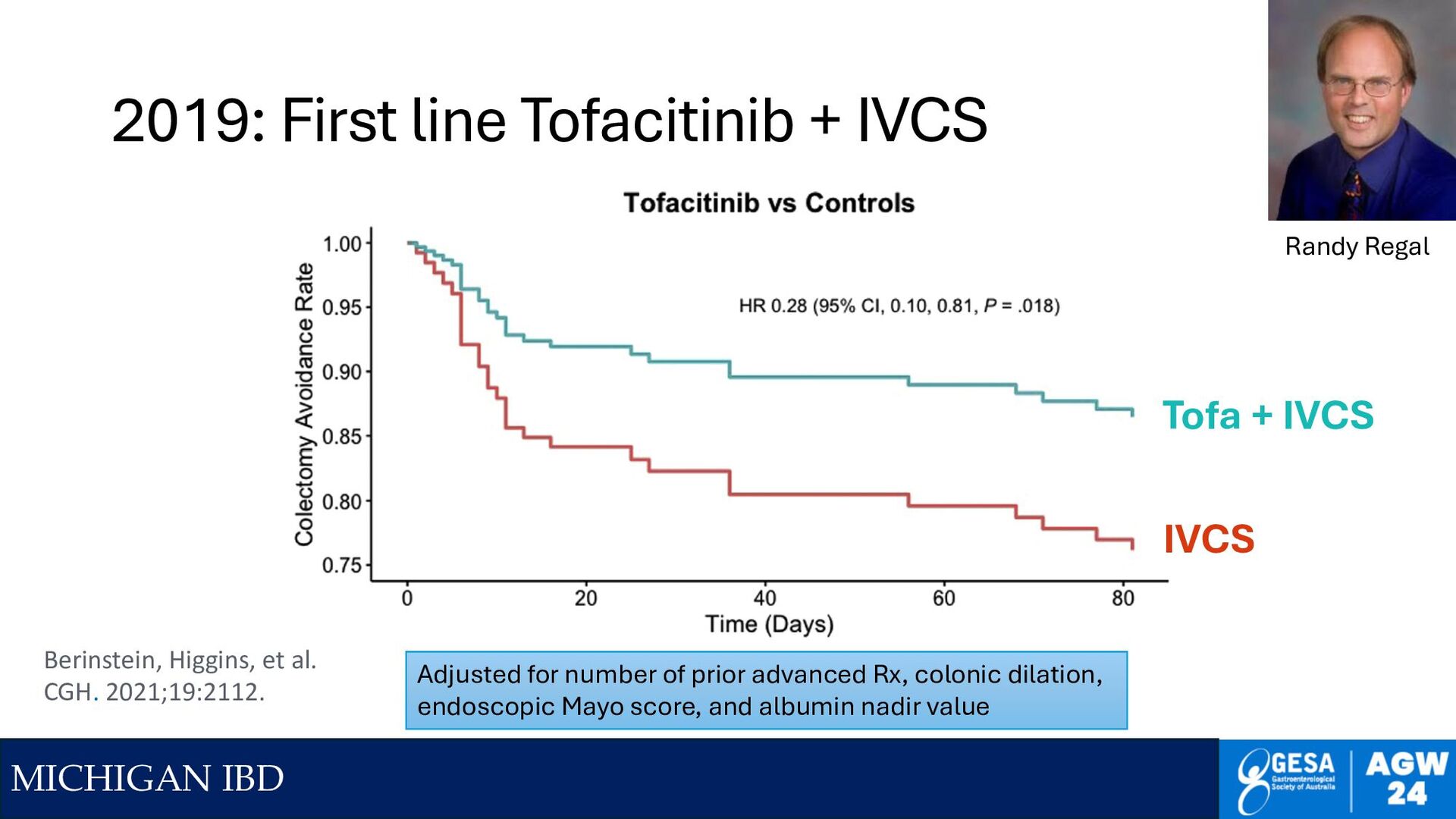
Tofa + IVCS IVCS Adjusted for number of prior advanced Rx, colonic dilation, endoscopic Mayo score, and albumin nadir value Berinstein, Higgins, et al. CGH. 2021;19:2112. Randy Regal
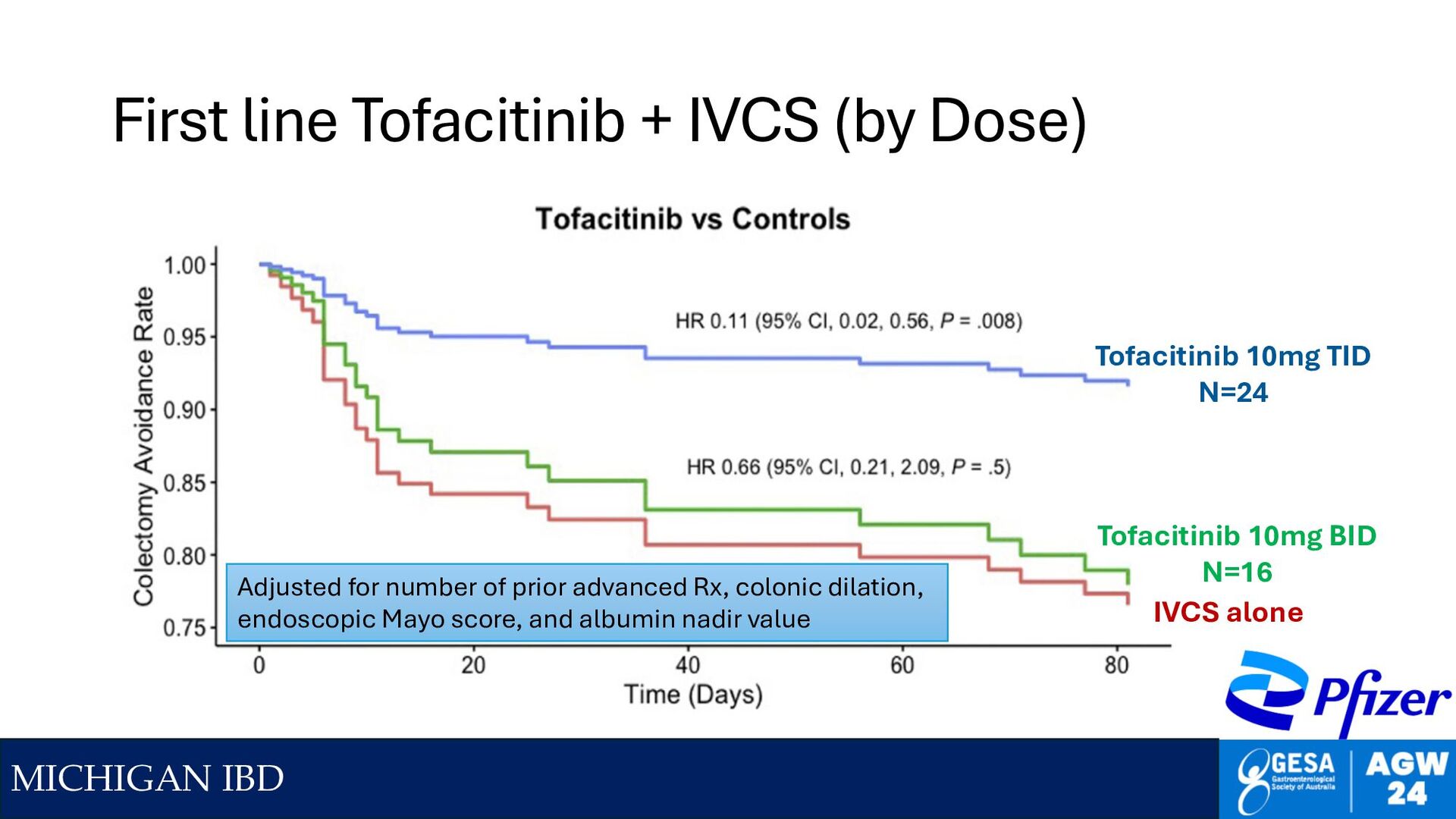
Dose) Tofacitinib 10mg TID N=24 IVCS alone Tofacitinib 10mg BID N=16 Adjusted for number of prior advanced Rx, colonic dilation, endoscopic Mayo score, and albumin nadir value
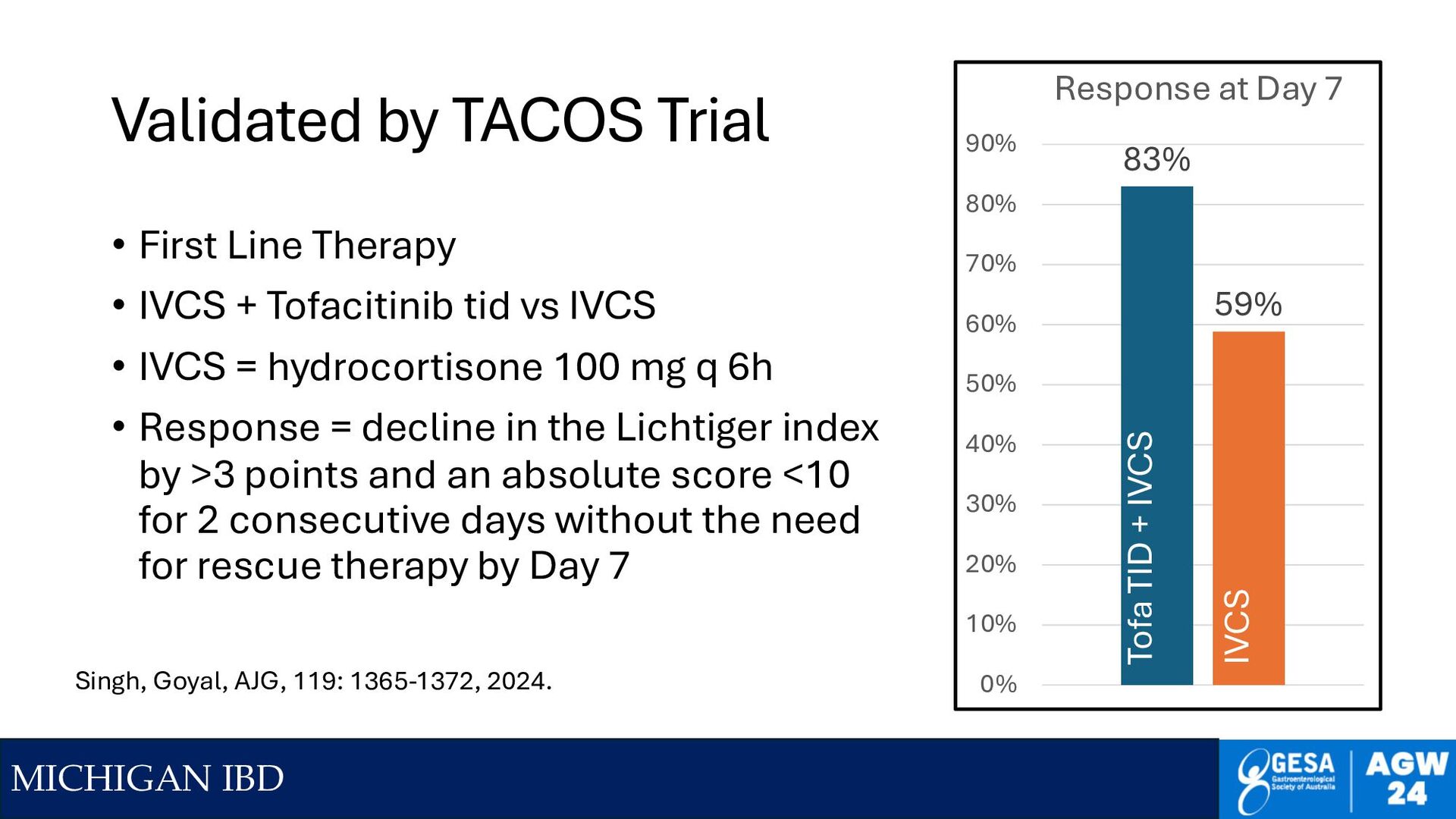
Line Therapy • IVCS + Tofacitinib tid vs IVCS • IVCS = hydrocortisone 100 mg q 6h • Response = decline in the Lichtiger index by >3 points and an absolute score <10 for 2 consecutive days without the need for rescue therapy by Day 7 83% 59% 0% 10% 20% 30% 40% 50% 60% 70% 80% 90% Response at Day 7 Tofa TID + IVCS IVCS Singh, Goyal, AJG, 119: 1365-1372, 2024.
with d5 Transition to 45 mg qd Upa x 8 weeks Berinstein, J., Higgins, PDR, et al Am J Gastro 2024;119:1421–1425 Upa + IVCS First Line IVCS First Line, IFX Rescue IVCS First Line, Monotherapy Adjusted for prior TNF use, CRP peak value, and albumin nadir value among patients at 5 centers since 2013
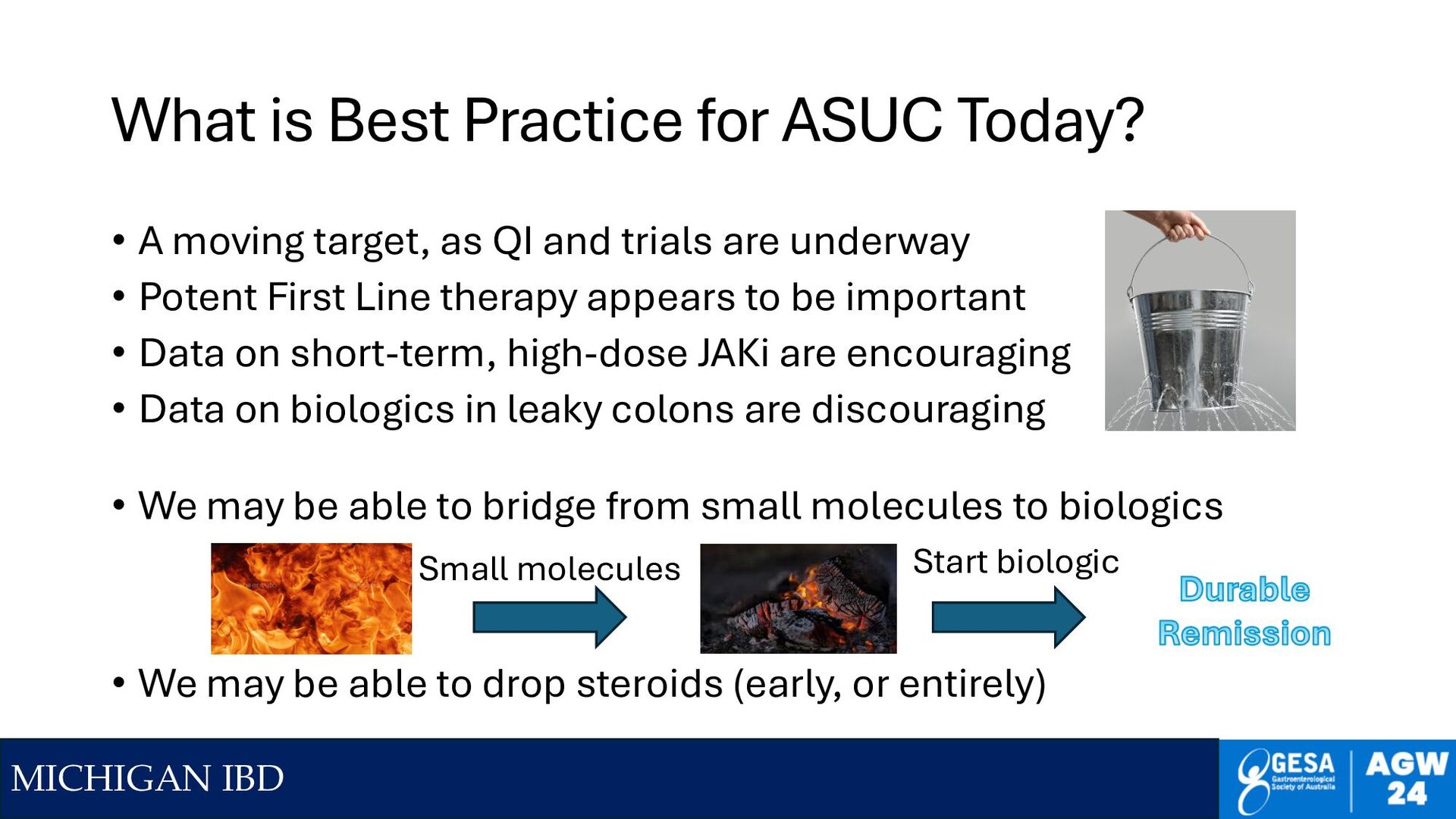
Today? • A moving target, as QI and trials are underway • Potent First Line therapy appears to be important • Data on short-term, high-dose JAKi are encouraging • Data on biologics in leaky colons are discouraging • We may be able to bridge from small molecules to biologics • We may be able to drop steroids (early, or entirely) Small molecules Start biologic
becomes leaky Gut immune cells exposed to luminal microbiome JAK/STAT activated • Cardioversion • Catheter RF ablation • We don't have Cardioverision for the colon • But can we (temporarily) ablate one part of the cycle?
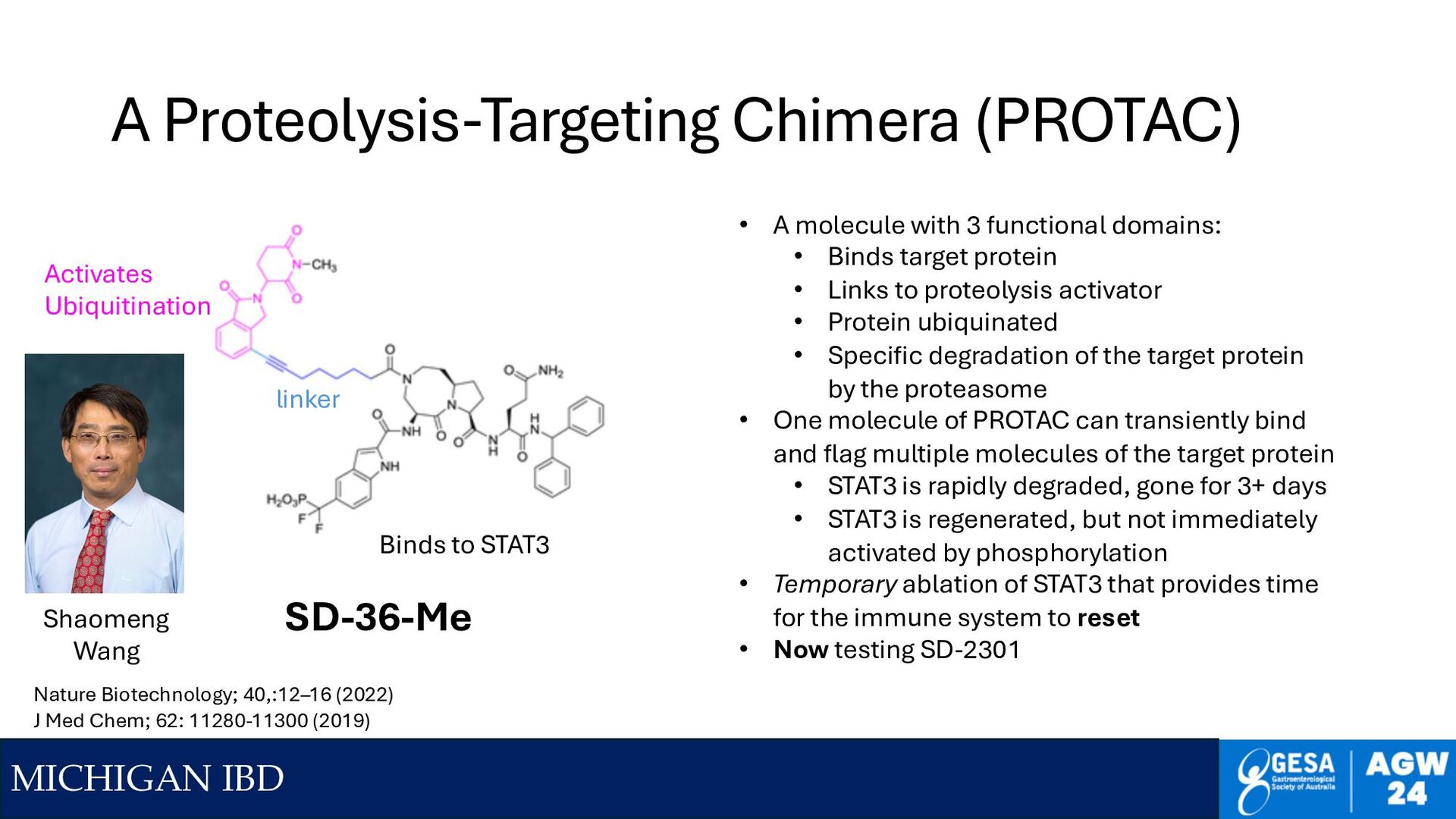
STAT3 linker Activates Ubiquitination • A molecule with 3 functional domains: • Binds target protein • Links to proteolysis activator • Protein ubiquinated • Specific degradation of the target protein by the proteasome • One molecule of PROTAC can transiently bind and flag multiple molecules of the target protein • STAT3 is rapidly degraded, gone for 3+ days • STAT3 is regenerated, but not immediately activated by phosphorylation • Temporary ablation of STAT3 that provides time for the immune system to reset • Now testing SD-2301 SD-36-Me Nature Biotechnology; 40,:12–16 (2022) J Med Chem; 62: 11280-11300 (2019) Shaomeng Wang
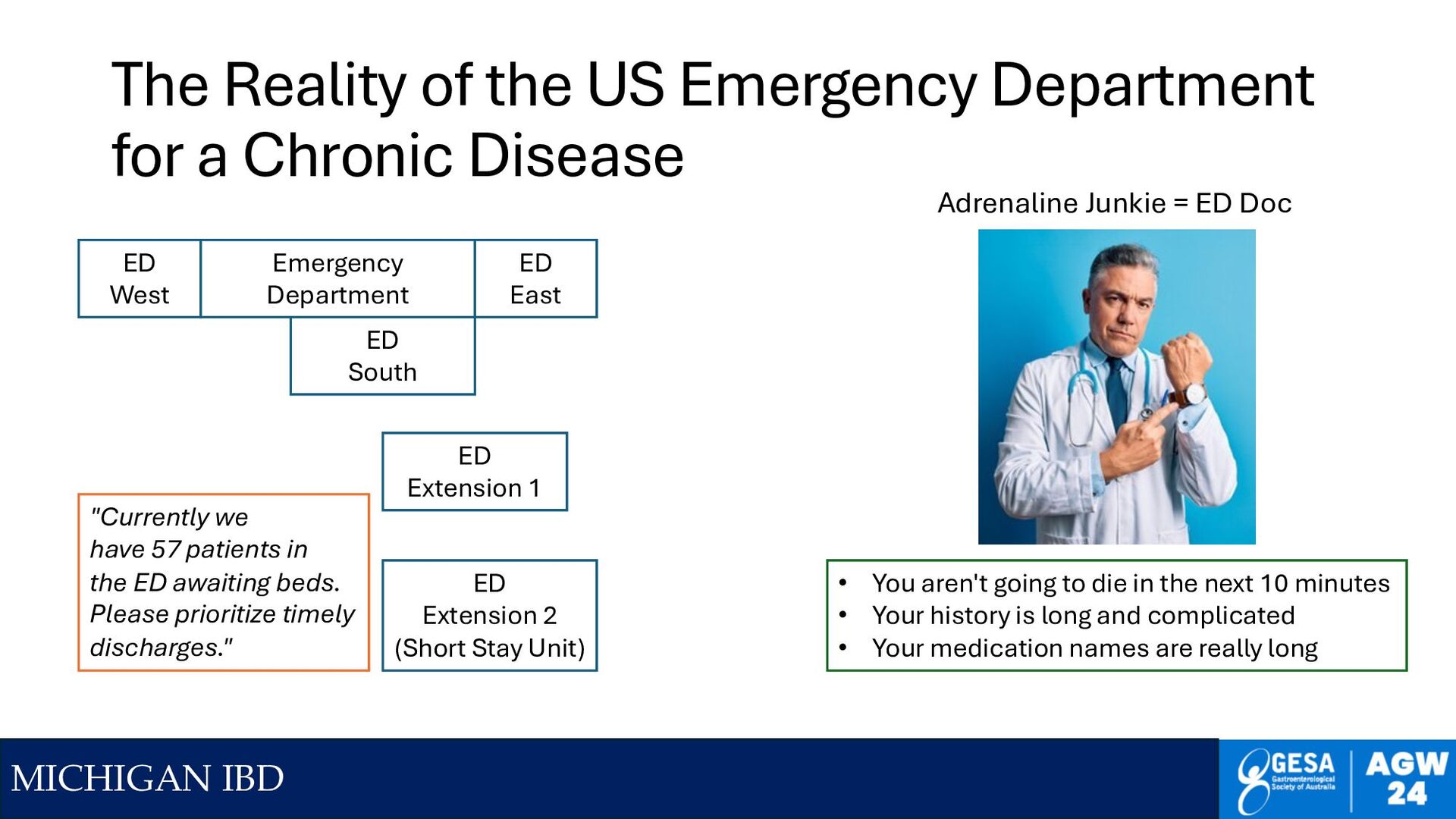
a Chronic Disease Emergency Department ED South ED West ED East ED Extension 1 ED Extension 2 (Short Stay Unit) "Currently we have 57 patients in the ED awaiting beds. Please prioritize timely discharges." • You aren't going to die in the next 10 minutes • Your history is long and complicated • Your medication names are really long Adrenaline Junkie = ED Doc
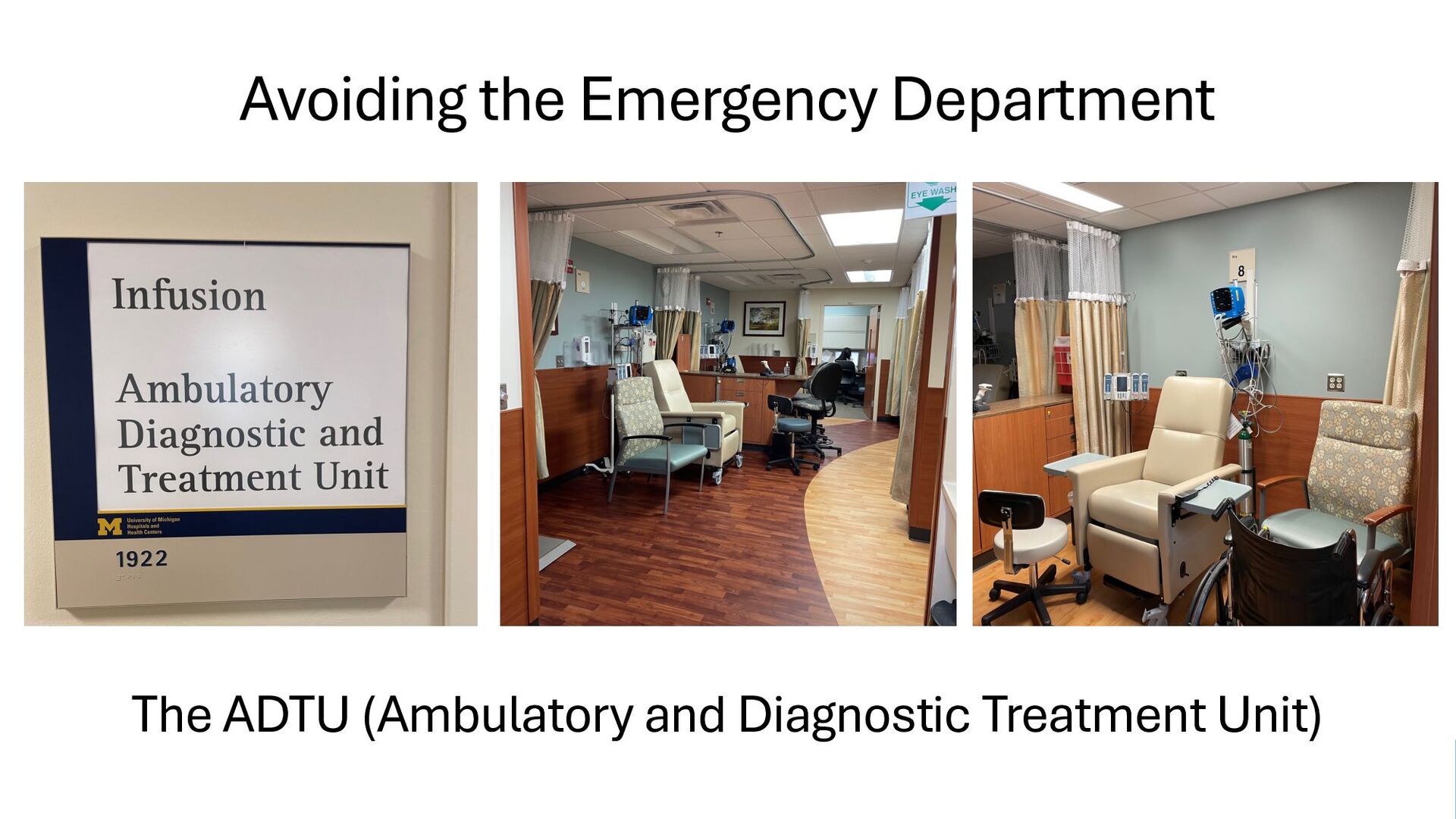
Staffed by Nurse Practitioners for flares of chronic diseases • Protocols for CHF, migraine, IBD, other diseases since 2017 • Patient calls with flare symptoms, appointment made for AM • Patient brings in stool, gets blood tests • Rapid FCP, CRP, GI PCR, CBC, Chem, (slower) drug levels • IV fluids, IVCS (possibly JAKi) per protocol • Consult with outpatient GI on next steps / change in maintenance • Option for CTE if needed • In and out within 5 hours
Started for ASUC in June 2024 at UMichigan • ASUC patients who have ‘turned the corner’ per criteria & physician • Typically 48-72h in hospital • Monitoring recovery curve • Go home with daily home nursing care • IV corticosteroids as needed • Daily Lab testing, Vitals • Daily PROs on mobile phone into EMR • Daily Zoom visits with physician • Can get outpt flex sig, X-ray, or return to GI service if a turn for the worse • Early experience: 40 km radius, 4/4 did well, big patient satisfaction
• Rebooting the immune system • Durable immunosuppression, infection, cancer? • To the ADTU instead of the Emergency Department • Will we miss emergencies? • Hospital Care at Home? • Will we be slow to bring patients back to the hospital when needed?
maximize first line Rx? Do we still need steroid tapers?/ Steroids at all? Do all ASUC patients need to be hospitalized? Can patients go home after day 2 with home nursing? Should we delay biologics until smoldering?
• Hypothesis: perioperative BB for noncardiac surgery • Lots of rapid publications • Led guidelines group, implemented BB in Europe • Other sites data ~ 27% increased mortality • Estimated 800K additional deaths in Europe • Many incentives and paths to research misconduct • External validation is critical • Believe in science, not your beloved hypothesis
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}