Rx Mechanisms of Action (MoA) • JAK, p19/p40, TNF, integrin *(not including S1P) • With MoA switching, can try 4 MoAs, then 6 possible dual combos • JAK-p19, JAK-integrin, JAK-TNF, p19-integrin, p19-TNF, TNF-integrin • Combos much more common with generic TNF, p40, and JAK by 2026 • Patients can have up to 10 options without repeating MoA before they get to clinical trials
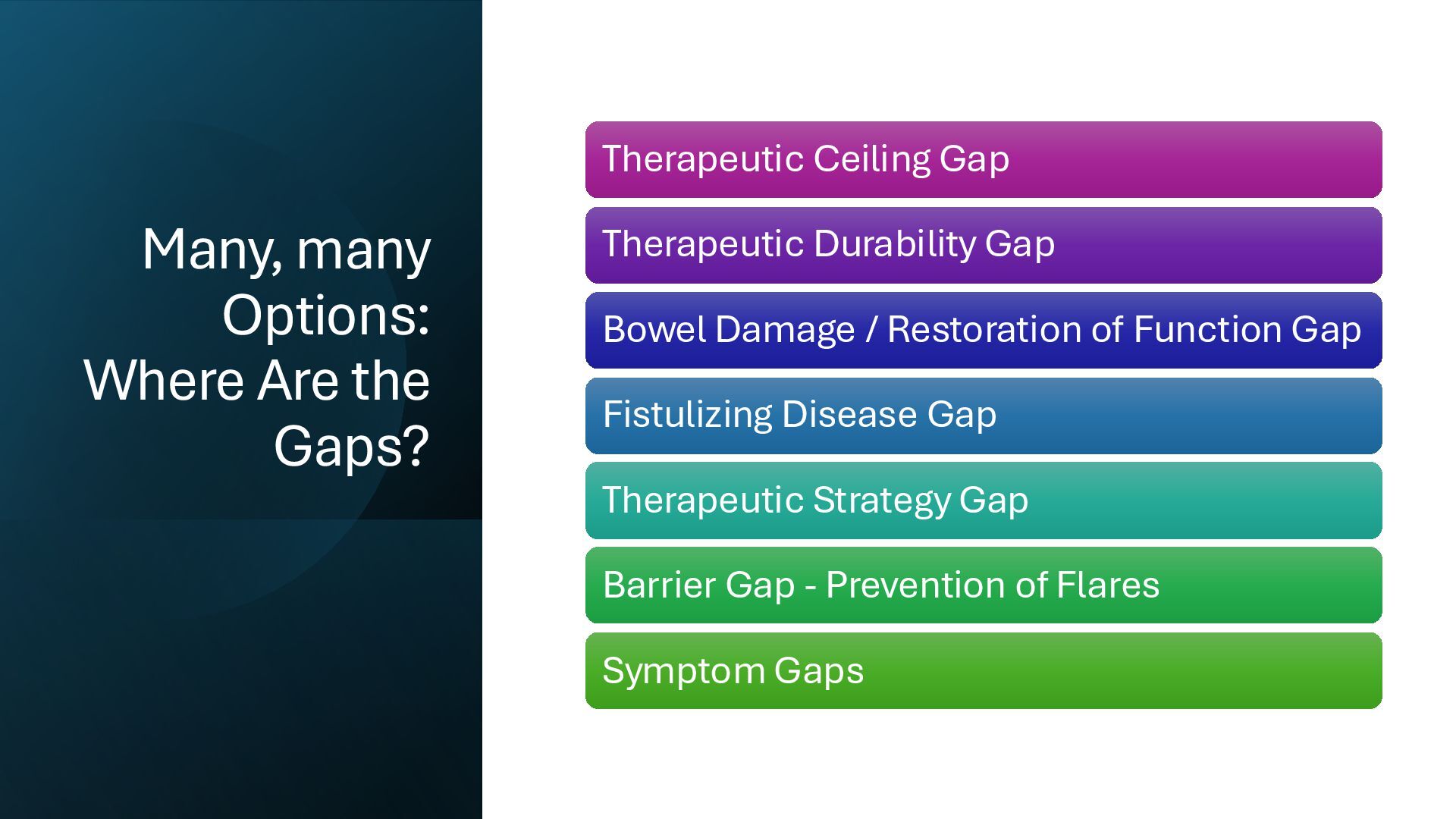
Therapeutic Durability Gap Bowel Damage / Restoration of Function Gap Fistulizing Disease Gap Therapeutic Strategy Gap Barrier Gap - Prevention of Flares Symptom Gaps
often feel like drug selection is trial and error • Essentially a spin of the wheel…. • Oftentimes limited by, or dictated by, their health insurance • Is there a better way to pick a therapy for a particular IBD patient?
Promise of Precision Medicine • Can we identify which inflammatory pathways are most important in this patient at this point in time? (which may change) • Genetics • Serologies • Mucosal biopsies/transcriptome? • Other factors? • And choose the best therapy for each patient?
anti-inflammatory monotherapies? EXL01 in Crohn's Disease – Wednesday PM Fighting back with bacteriophage – Thursday AM Live biotherapeutic – Thursday AM
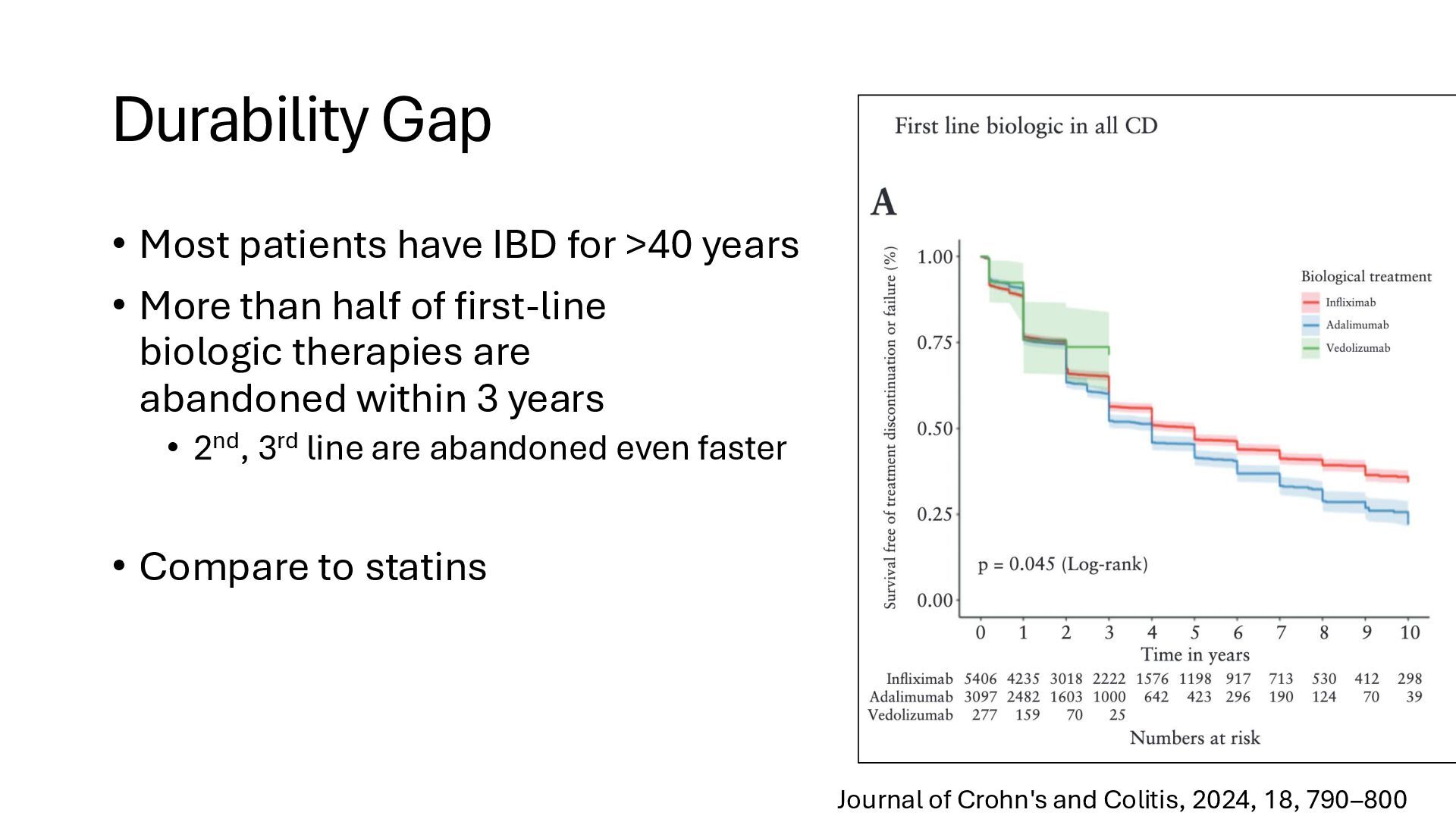
• More than half of first-line biologic therapies are abandoned within 3 years • 2nd, 3rd line are abandoned even faster • Compare to statins Journal of Crohn's and Colitis, 2024, 18, 790–800
with nasal spray delivery of biologic + IL-10 to induce tolerance to the biologic? • Focus on maintenance biologics after small molecule induction for less leak? • Disguise the foreign proteins? • Continuous release? Thursday AM The Dream: IBD therapies that keep working for 40+ Years
Loss of barrier function with creeping fat as a patch • Fibrosis, muscle hypertrophy, loss of accomodation (stretch) • Increased neuroenteric sensitivity Restoration of Function • Rx to improve barrier function • ALK5i. Axli, Bcl2i • Anti-fibrotics • Turn down enteric sensitivity?
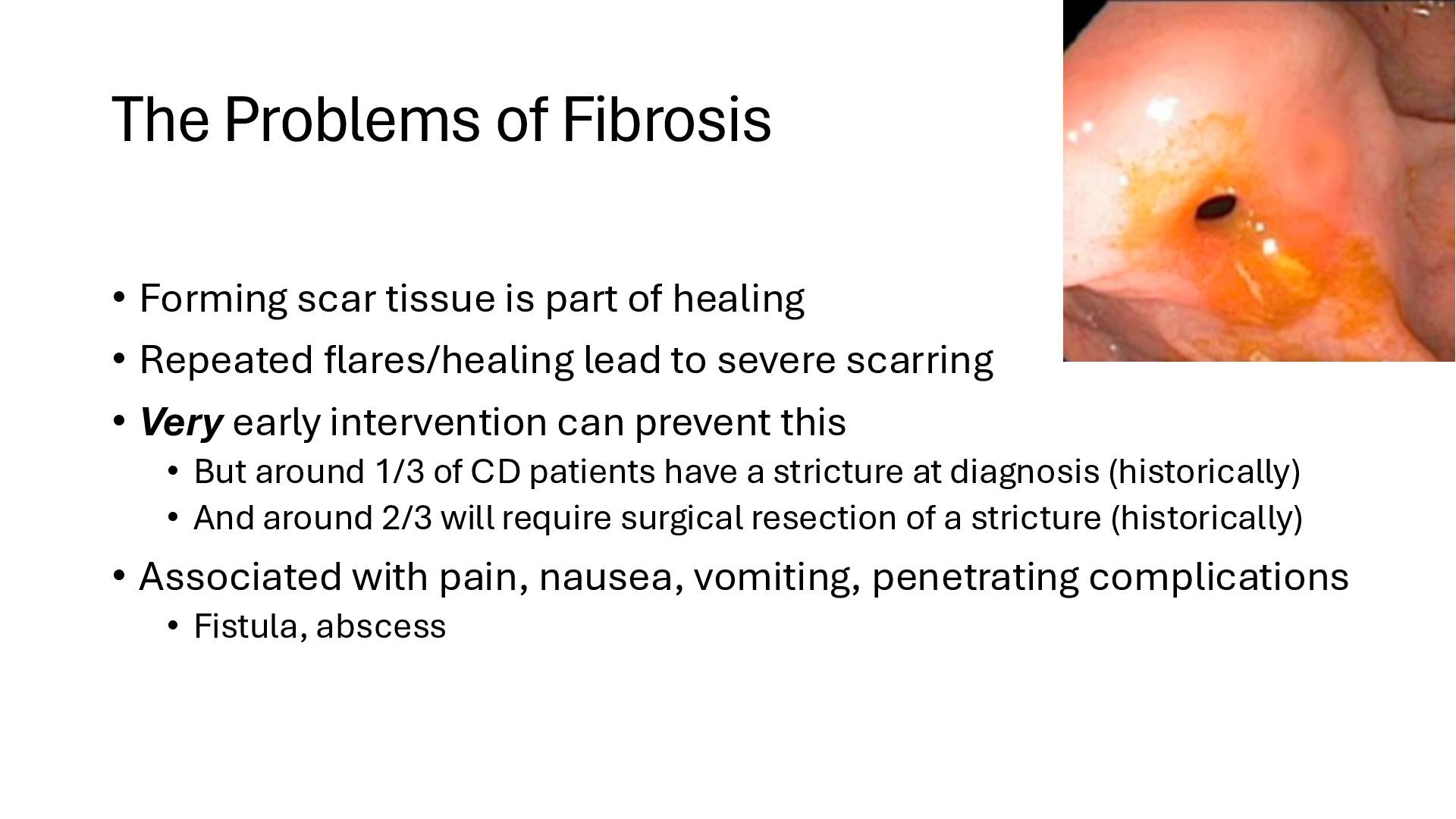
of healing • Repeated flares/healing lead to severe scarring • Very early intervention can prevent this • But around 1/3 of CD patients have a stricture at diagnosis (historically) • And around 2/3 will require surgical resection of a stricture (historically) • Associated with pain, nausea, vomiting, penetrating complications • Fistula, abscess
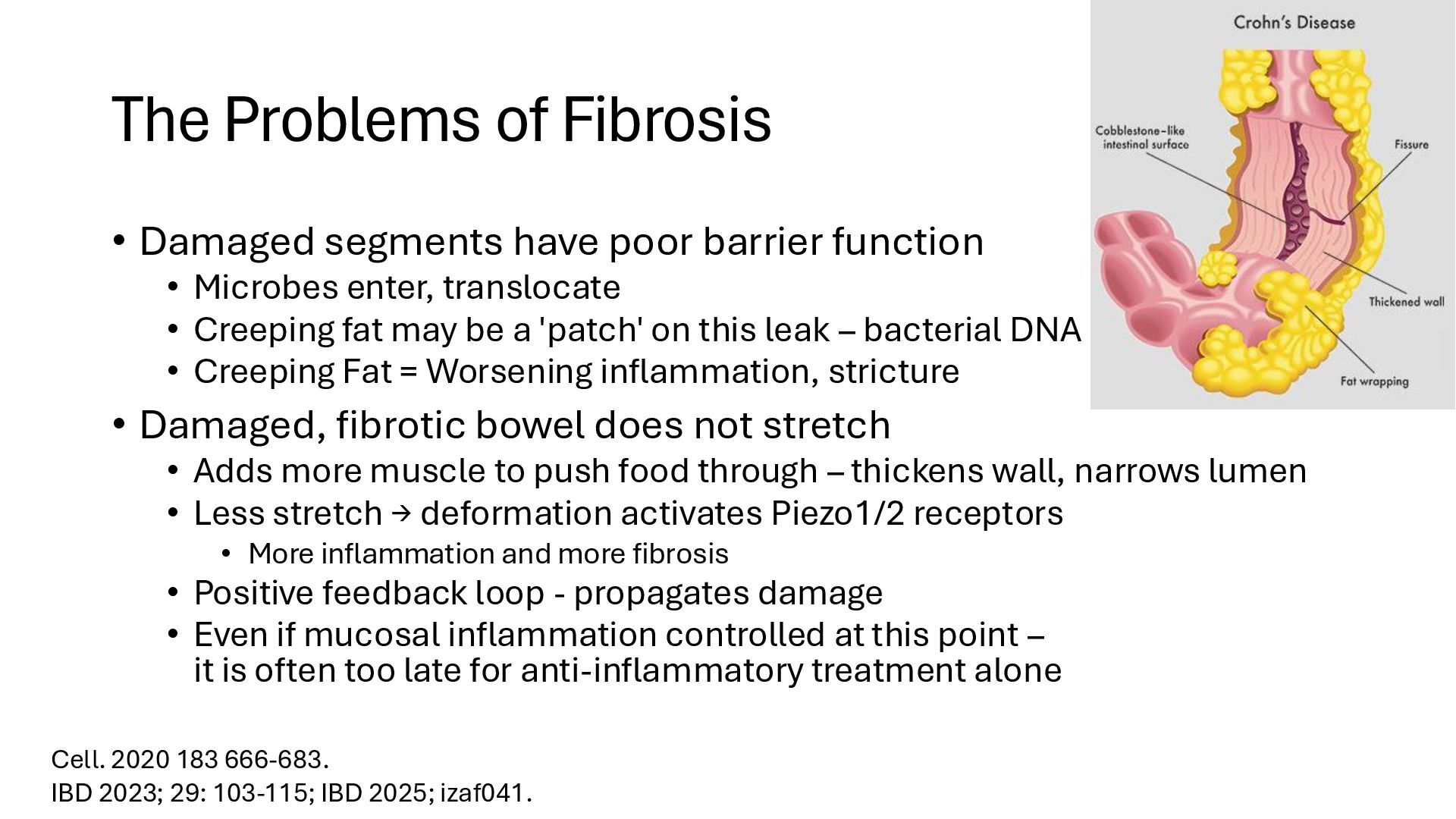
function • Microbes enter, translocate • Creeping fat may be a 'patch' on this leak – bacterial DNA • Creeping Fat = Worsening inflammation, stricture • Damaged, fibrotic bowel does not stretch • Adds more muscle to push food through – thickens wall, narrows lumen • Less stretch → deformation activates Piezo1/2 receptors • More inflammation and more fibrosis • Positive feedback loop - propagates damage • Even if mucosal inflammation controlled at this point – it is often too late for anti-inflammatory treatment alone Cell. 2020 183 666-683. IBD 2023; 29: 103-115; IBD 2025; izaf041.
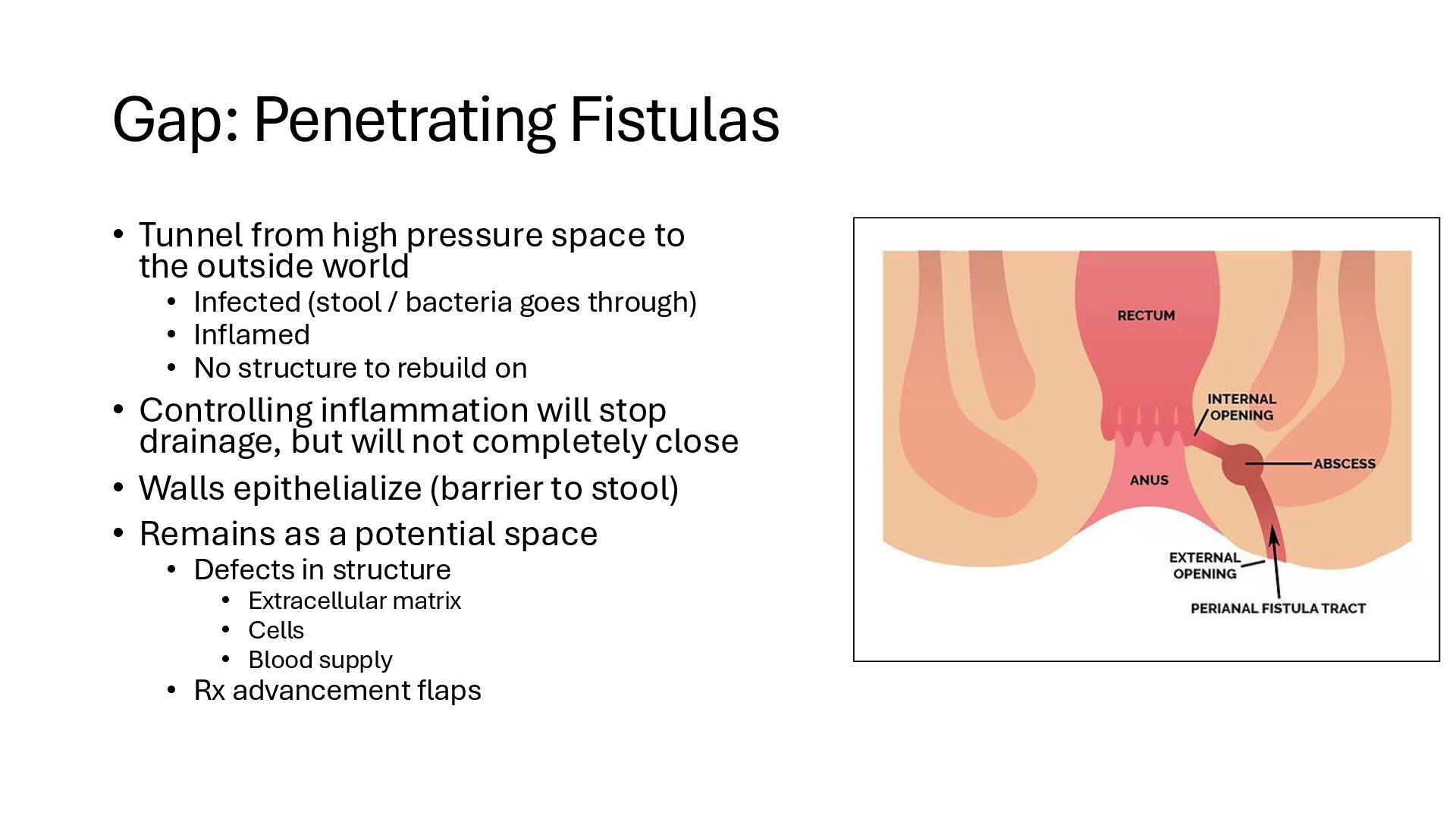
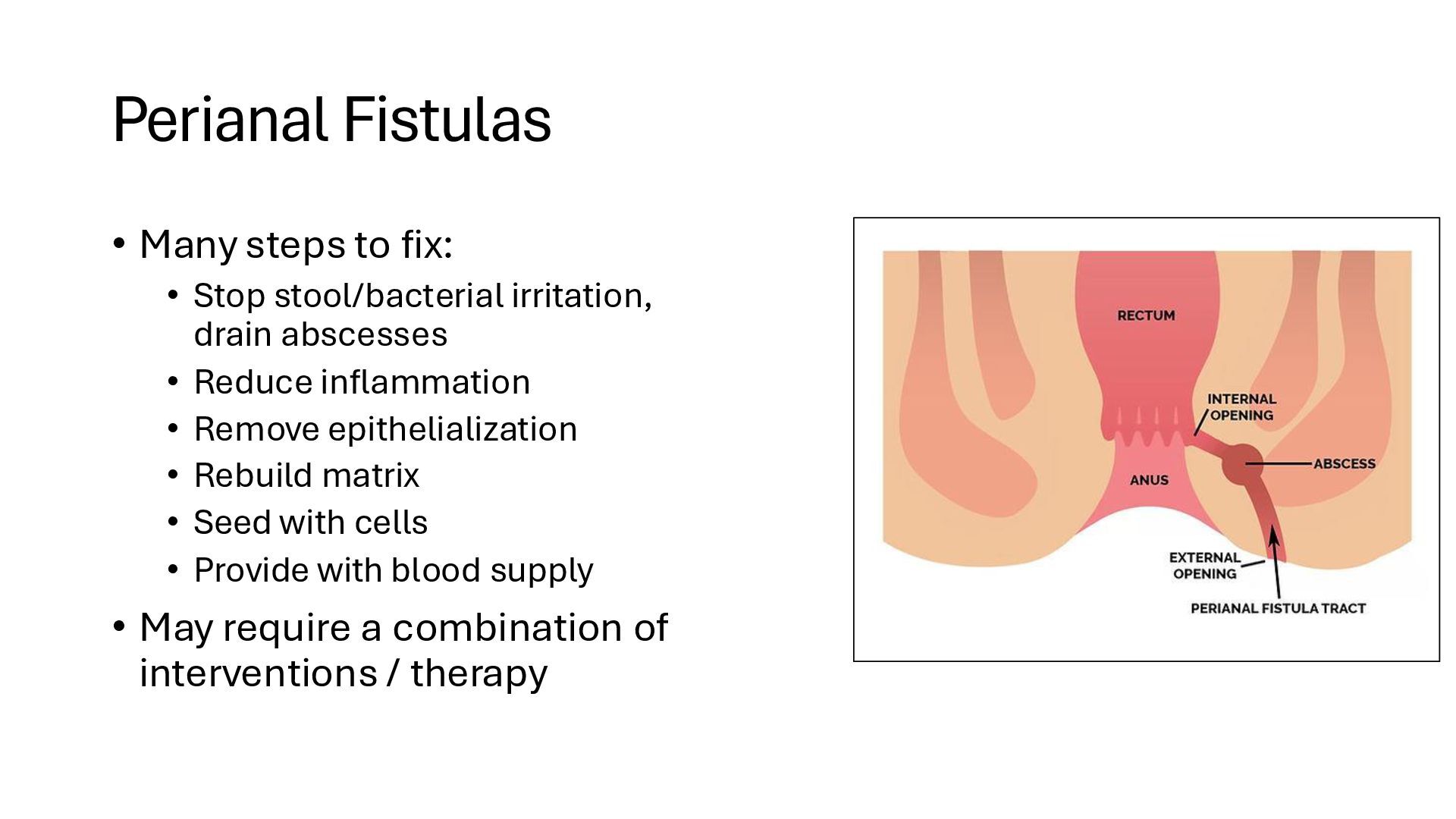
the outside world • Infected (stool / bacteria goes through) • Inflamed • No structure to rebuild on • Controlling inflammation will stop drainage, but will not completely close • Walls epithelialize (barrier to stool) • Remains as a potential space • Defects in structure • Extracellular matrix • Cells • Blood supply • Rx advancement flaps
irritation, drain abscesses • Reduce inflammation • Remove epithelialization • Rebuild matrix • Seed with cells • Provide with blood supply • May require a combination of interventions / therapy
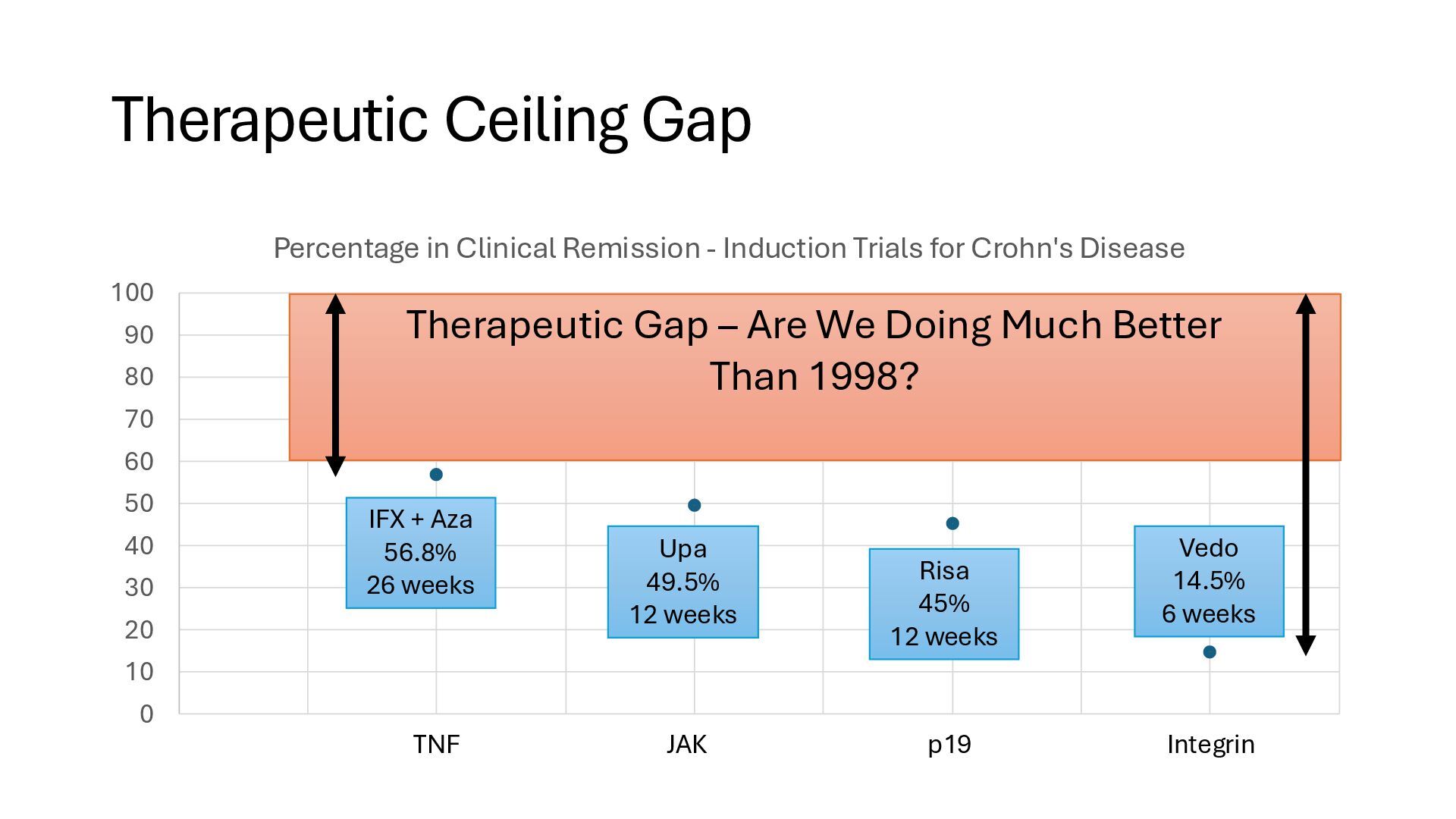
approval • Not on how to best use a drug • Better than placebo is a very low bar • Infliximab • 1998 - approved, used as single dose, often in-hospital • 2002 - establish need for maintenance (avoid anti-IFX Abs) • 2010 - establish superiority of IFX/Aza combo • 2015 - understand intestinal drug leak • Avoid initiation during severe flare with low Albumin Lancet. 2002; 359: 1541-9. N Engl J Med 2010;362:1383-139. Gastroenterology. 2015 Aug;149(2):350-5.
• Prevent bowel damage, steroids, surgeries • Close monitoring • Early intervention before clinical flares occur • Start biologics (leak sensitive) when smoldering, not inferno • Need sequencing trials of small molecules first, then biologic • Cell therapies • CAR-T has been remarkably successful for cancers • Early positive results for B-cell based rheumatologic diseases (SLE, SSc) • Can T cell-directed therapies (BMT, Treg) produce a durable cure? • Antibody Conjugates • We can target, but can we deliver?
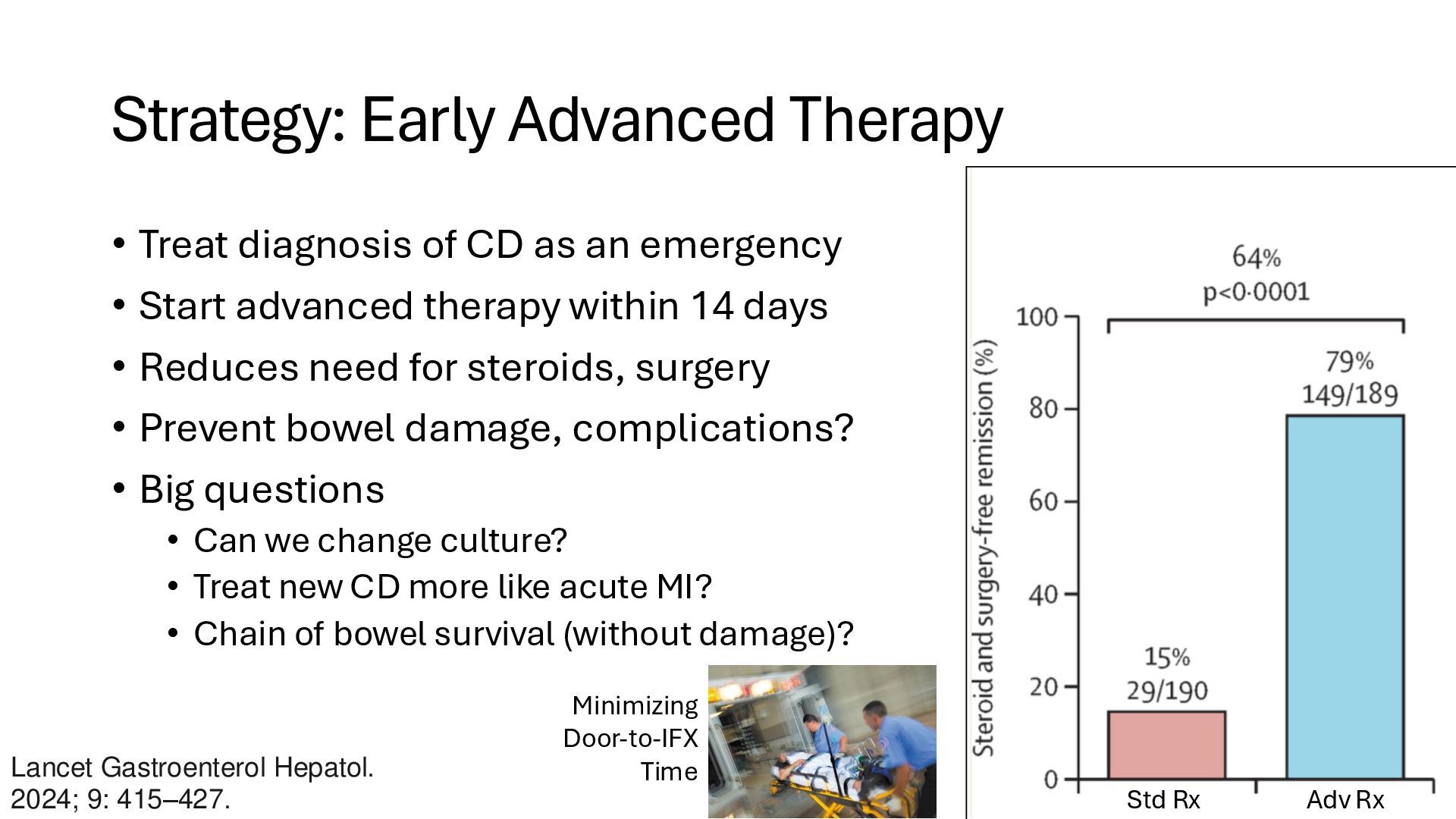
an emergency • Start advanced therapy within 14 days • Reduces need for steroids, surgery • Prevent bowel damage, complications? • Big questions • Can we change culture? • Treat new CD more like acute MI? • Chain of bowel survival (without damage)? Lancet Gastroenterol Hepatol. 2024; 9: 415–427. Std Rx Adv Rx Minimizing Door-to-IFX Time
smolder slowly long before a symptomatic flare starts • How to monitor inflammation, barrier function between visits? • How can we monitor closely to intercept flares early? • Frequent Blood or Stool Samples • Biometrics – sleep, steps, HR, etc. • Sweat Calprotectin - Enlisense (IBD Ventures) Rapid monitoring Thursday AM
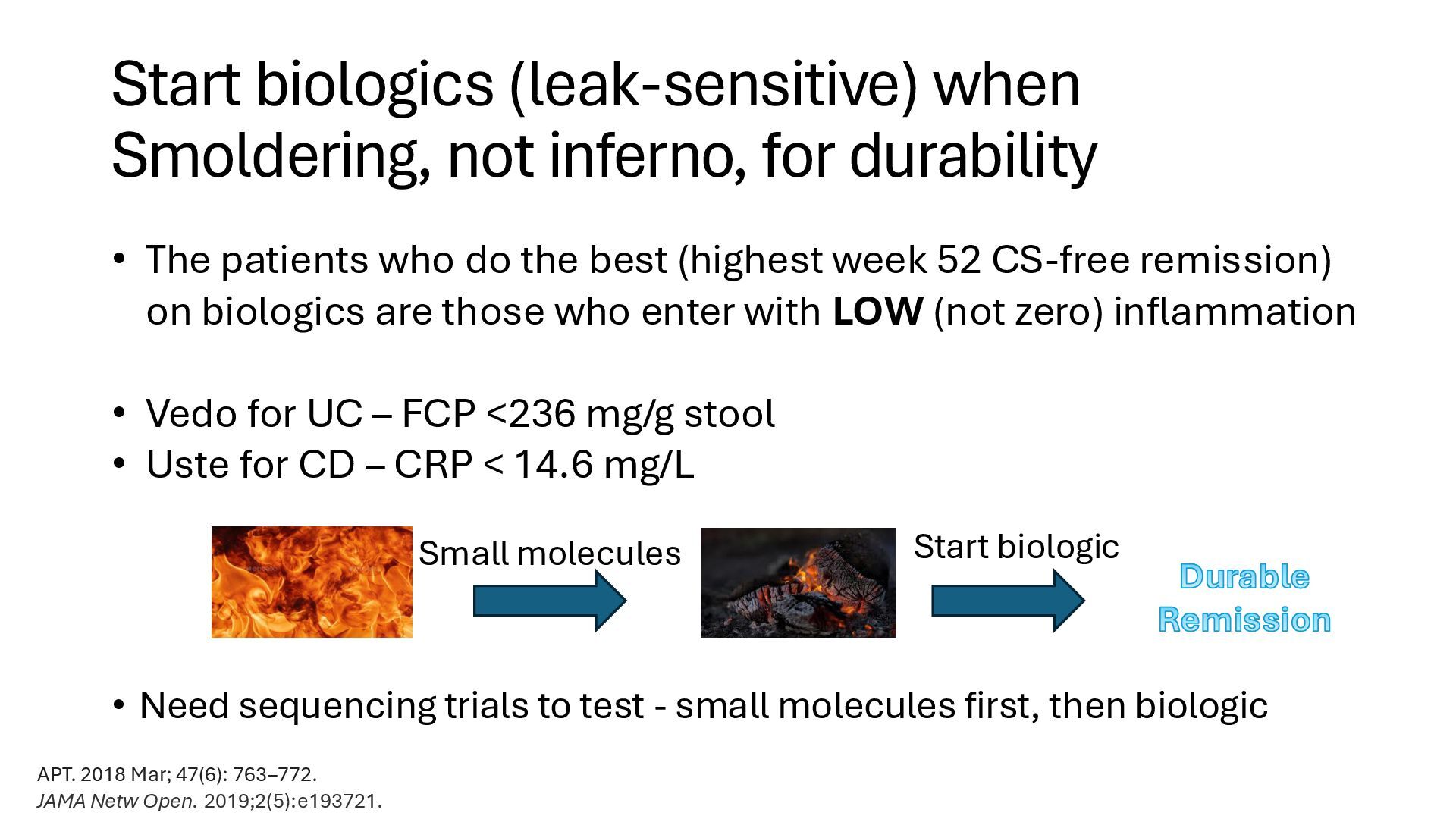
Need sequencing trials to test - small molecules first, then biologic Small molecules Start biologic Durable Remission APT. 2018 Mar; 47(6): 763–772. JAMA Netw Open. 2019;2(5):e193721. • The patients who do the best (highest week 52 CS-free remission) on biologics are those who enter with LOW (not zero) inflammation • Vedo for UC – FCP <236 mg/g stool • Uste for CD – CRP < 14.6 mg/L
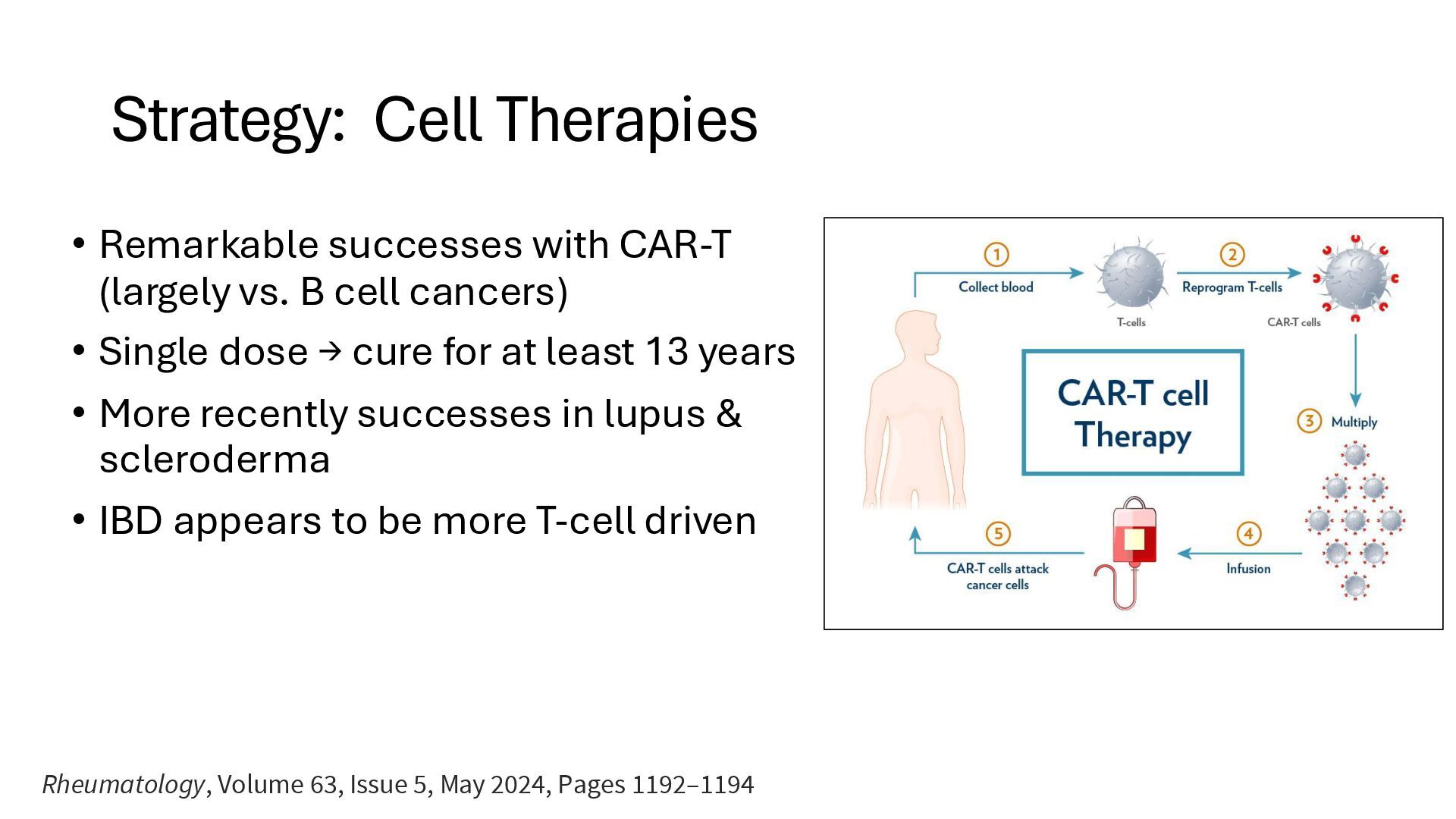
B cell cancers) • Single dose → cure for at least 13 years • More recently successes in lupus & scleroderma • IBD appears to be more T-cell driven Rheumatology, Volume 63, Issue 5, May 2024, Pages 1192–1194
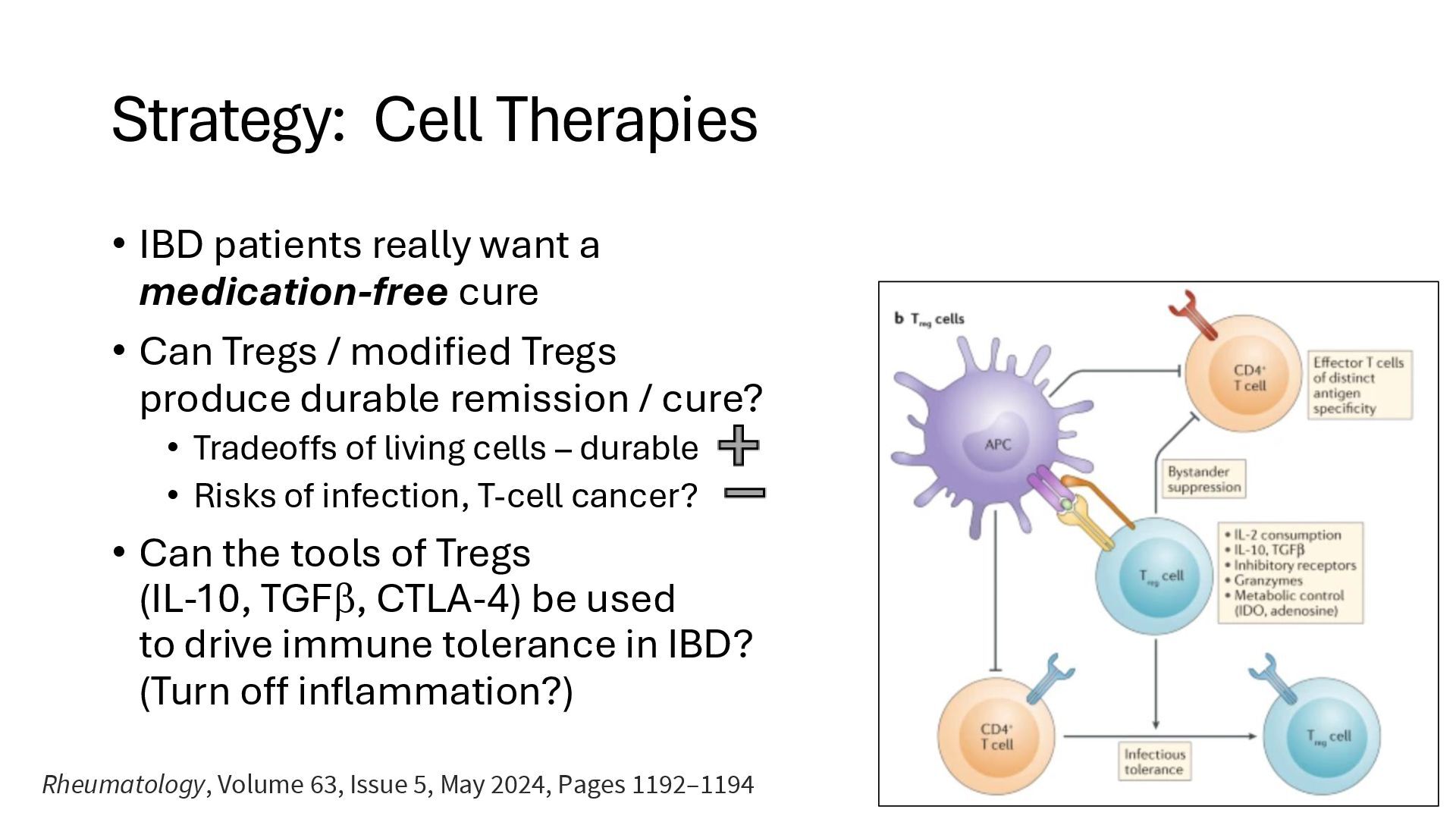
cure • Can Tregs / modified Tregs produce durable remission / cure? • Tradeoffs of living cells – durable • Risks of infection, T-cell cancer? • Can the tools of Tregs (IL-10, TGF, CTLA-4) be used to drive immune tolerance in IBD? (Turn off inflammation?) Rheumatology, Volume 63, Issue 5, May 2024, Pages 1192–1194
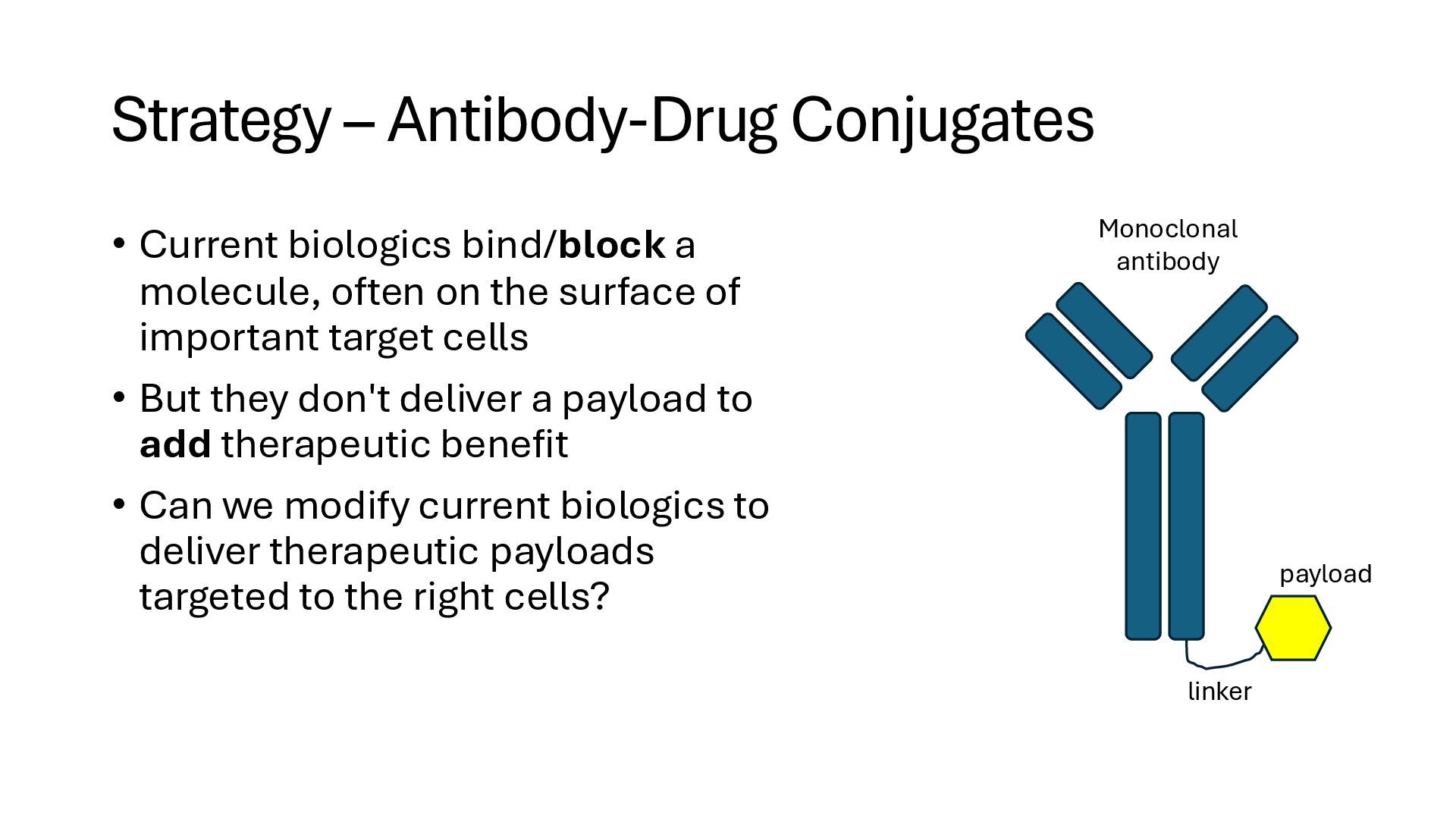
often on the surface of important target cells • But they don't deliver a payload to add therapeutic benefit • Can we modify current biologics to deliver therapeutic payloads targeted to the right cells? linker payload Monoclonal antibody
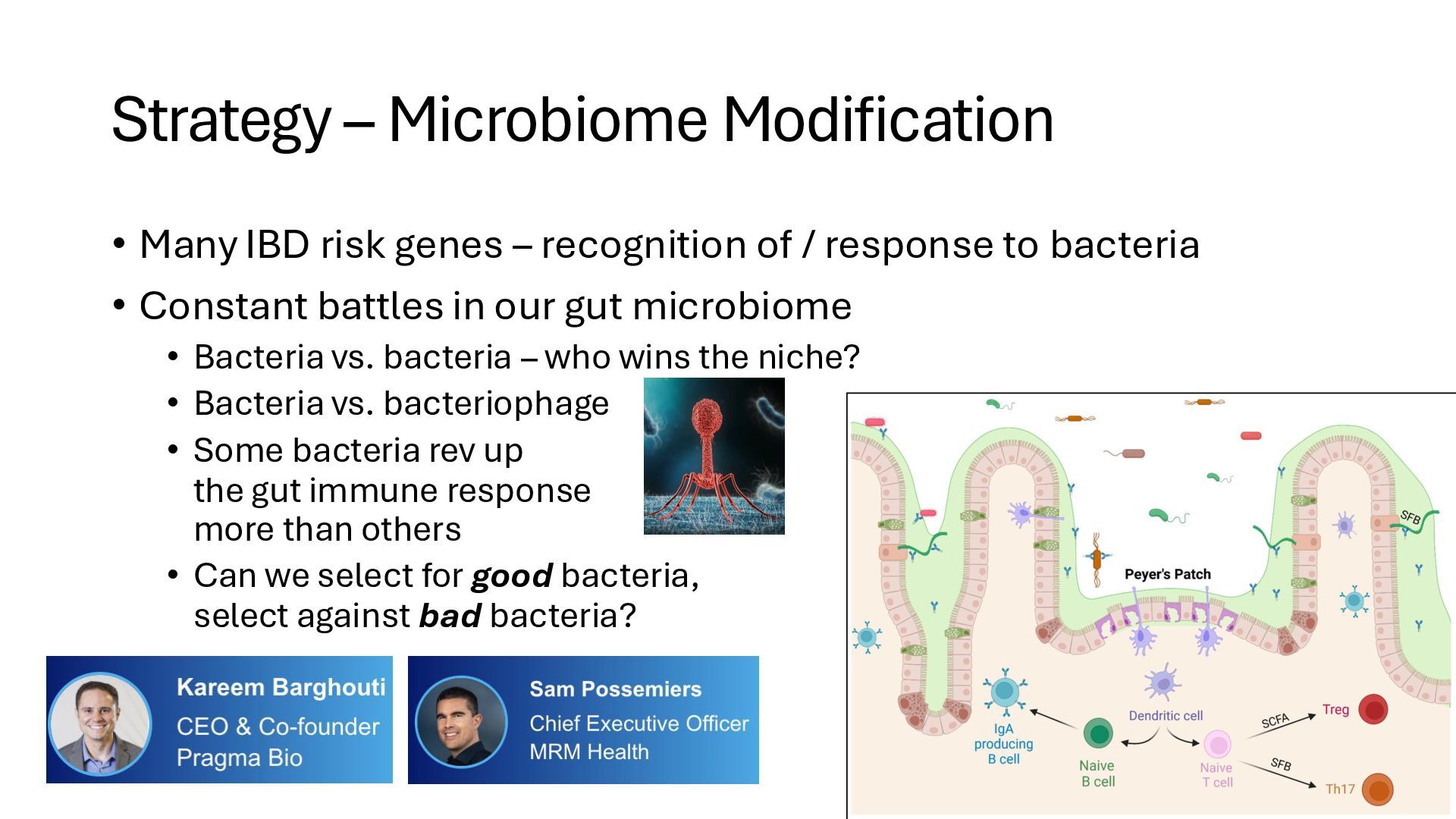
recognition of / response to bacteria • Constant battles in our gut microbiome • Bacteria vs. bacteria – who wins the niche? • Bacteria vs. bacteriophage • Some bacteria rev up the gut immune response more than others • Can we select for good bacteria, select against bad bacteria?
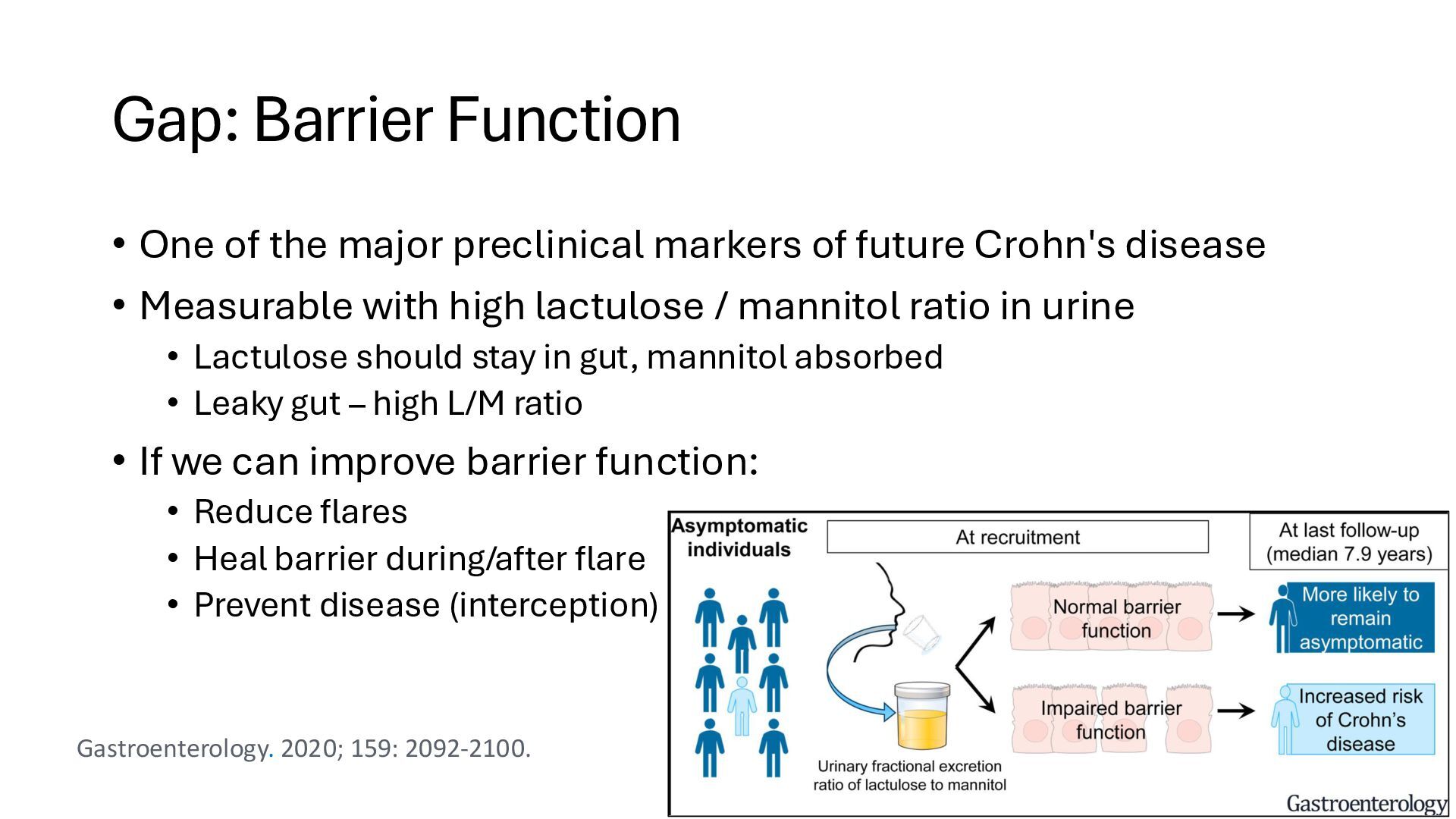
of future Crohn's disease • Measurable with high lactulose / mannitol ratio in urine • Lactulose should stay in gut, mannitol absorbed • Leaky gut – high L/M ratio • If we can improve barrier function: • Reduce flares • Heal barrier during/after flare • Prevent disease (interception) Gastroenterology. 2020; 159: 2092-2100.
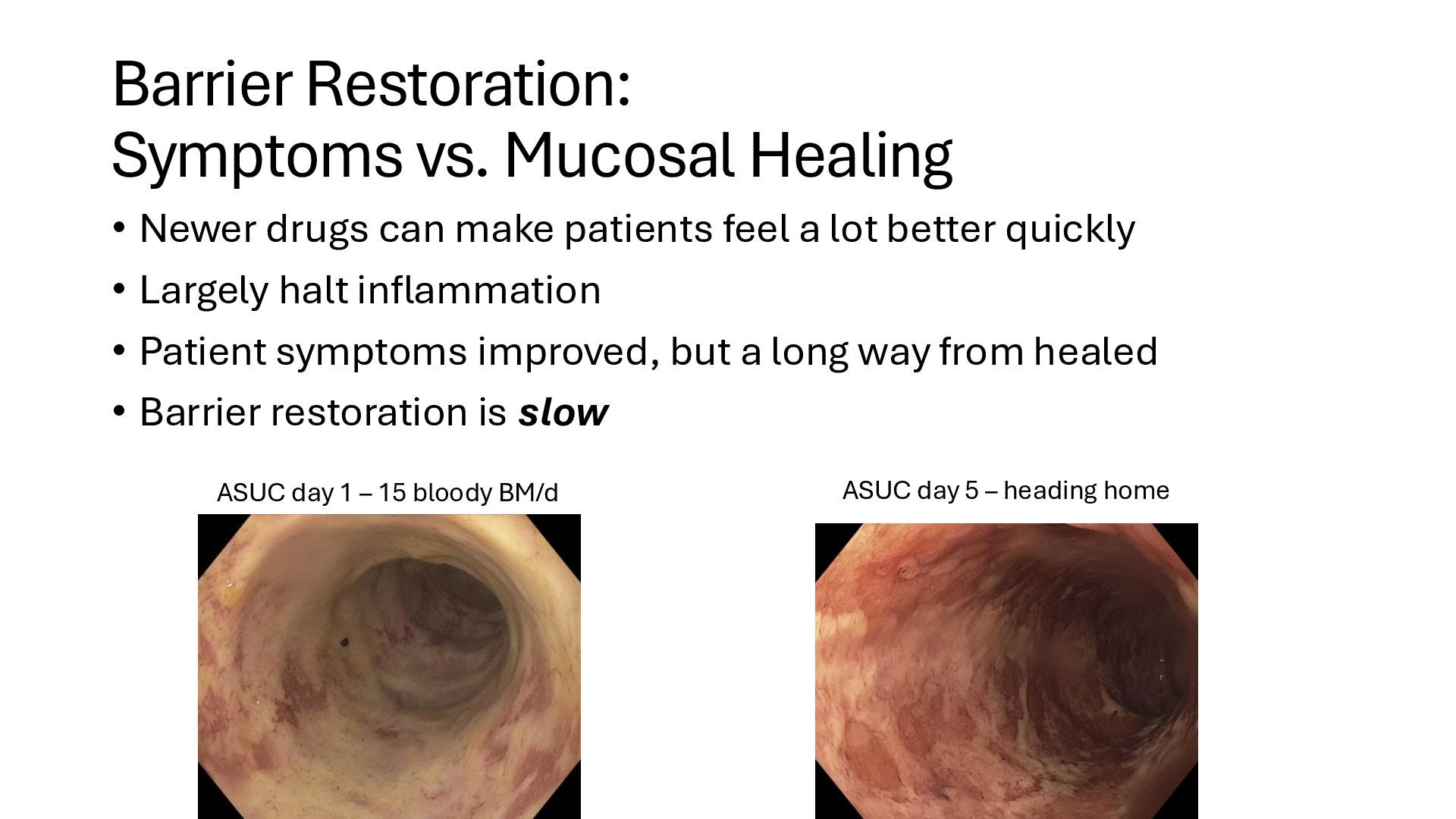
make patients feel a lot better quickly • Largely halt inflammation • Patient symptoms improved, but a long way from healed • Barrier restoration is slow ASUC day 1 – 15 bloody BM/d ASUC day 5 – heading home
damage • Serum, mucosal, and stool PAI-1 associated with active IBD • PAI-1 inhibitors in development (IBD Ventures) • GPR35 agonists • An orphan G protein coupled receptor • Agonists of GPR35 promote wound repair of gut epithelium • Thursday afternoon – ThirtyFiveBio Sci Transl Med 2019; 11: eeat0852 J Crohns Colitis. 2024 Mar 1;18(3):392-405.
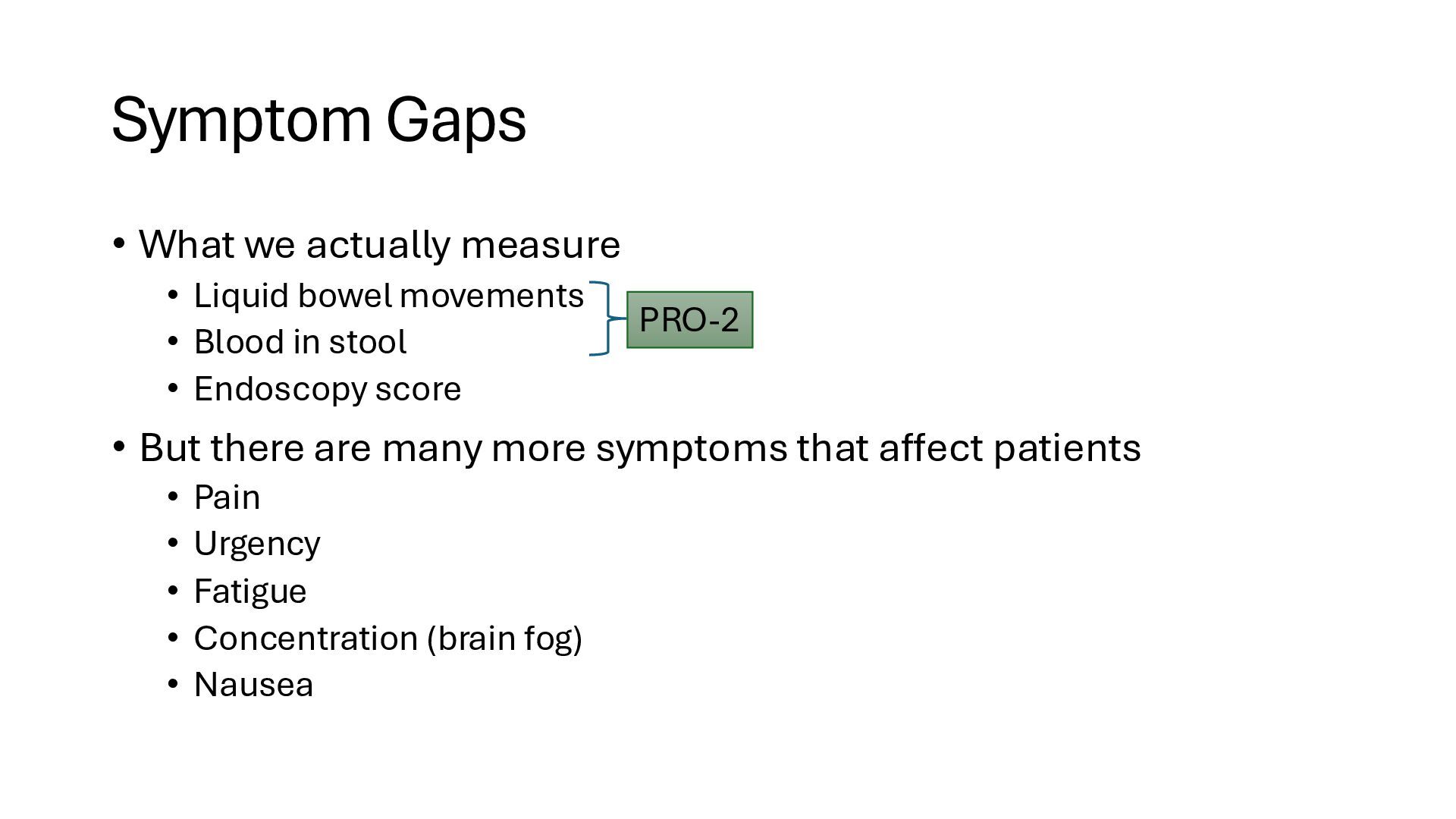
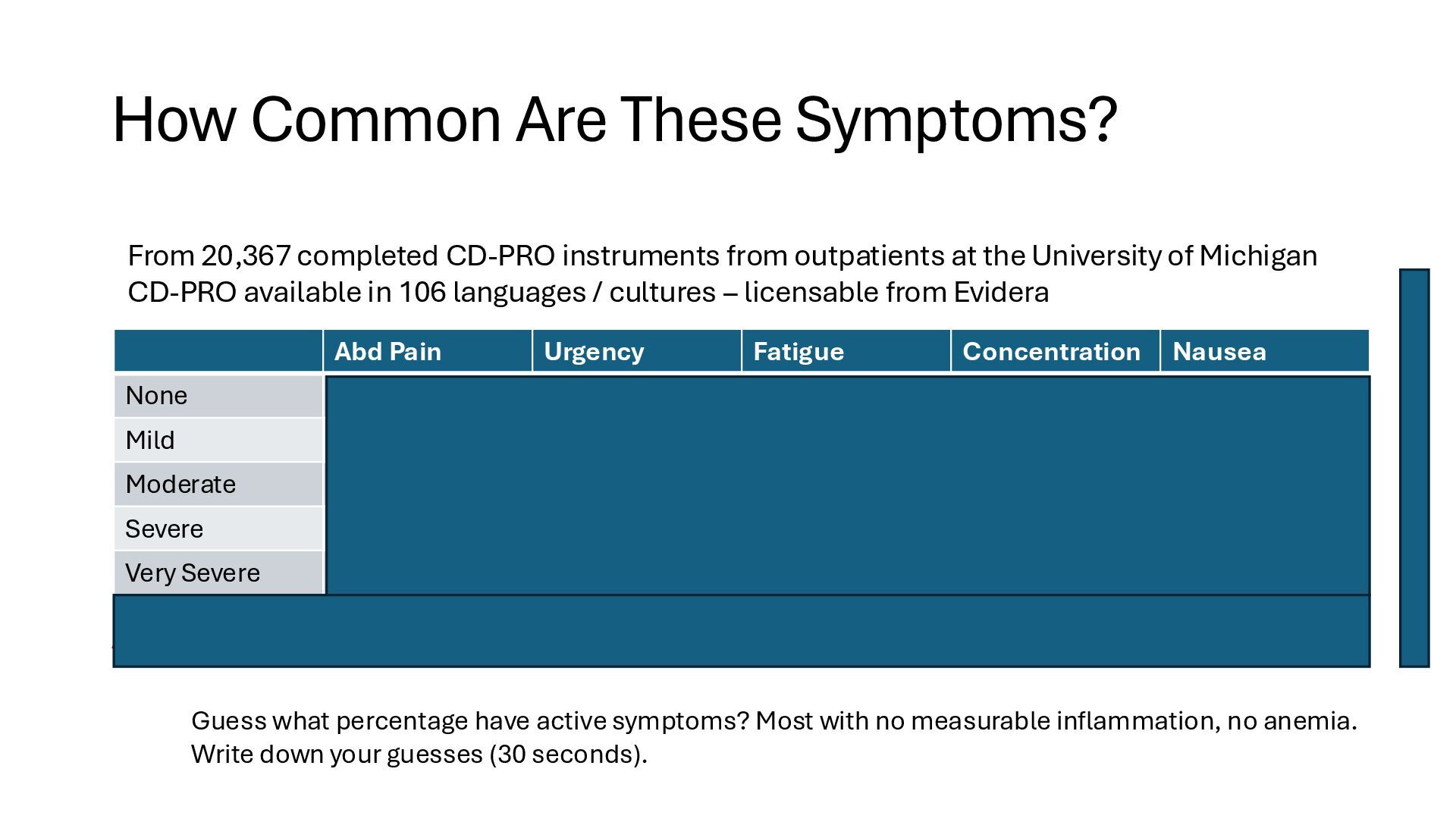
movements • Blood in stool • Endoscopy score • But there are many more symptoms that affect patients • Pain • Urgency • Fatigue • Concentration (brain fog) • Nausea PRO-2
Nausea None 10,367 (50.1%) 8,429 (40.7%) 4,788 (23.1%) 11,939 (57.7%) 13,961 (67.5%) Mild 5,586 (27%) 5,110 (24.7%) 6,723 (32.4%) 4,390 (21.2%) 3,695 (17.9%) Moderate 3,505 (16.9%) 4,136 (19.9%) 6,028 (29.1%) 2,454 (11.9%) 1,992 (9.6%) Severe 955 (4.6%) 2,089 (10%) 2,296 (11.1%) 1,257 (6.1%) 797 (3.9%) Very Severe 274 (1.3%) 923 (4.5%) 852 (4.1%) 647 (3.1%) 242 (1.1%) From 20,367 completed CD-PRO instruments from outpatients at the University of Michigan CD-PRO available in 106 languages / cultures – licensable from Evidera 49.9% 59.3% 76.9% 42.3% 32.5% Active Symptom Guess what percentage have active symptoms? Most with no measurable inflammation, no anemia. Write down your guesses (30 seconds).
in IBD is nearly 50% despite Rx • Use of Narcotics in IBD in the US • 21% of outpatients and 62% of inpatients use narcotics for pain in IBD • Lots of issues with addiction and overdose in chronic diseases • Problems with nonselective NSAIDs • Considered to increase the risk of IBD relapse (retrospective) • Believed to be due to dual Cox 1 & 2 inhibition – coxibs safer? • Our two go-to pain medication categories are problematic in IBD CGH 2021; 19:985 Dig Dis Sci 2006; 51: 168-72; Clin Gast Hep 2006; 4: 196-202
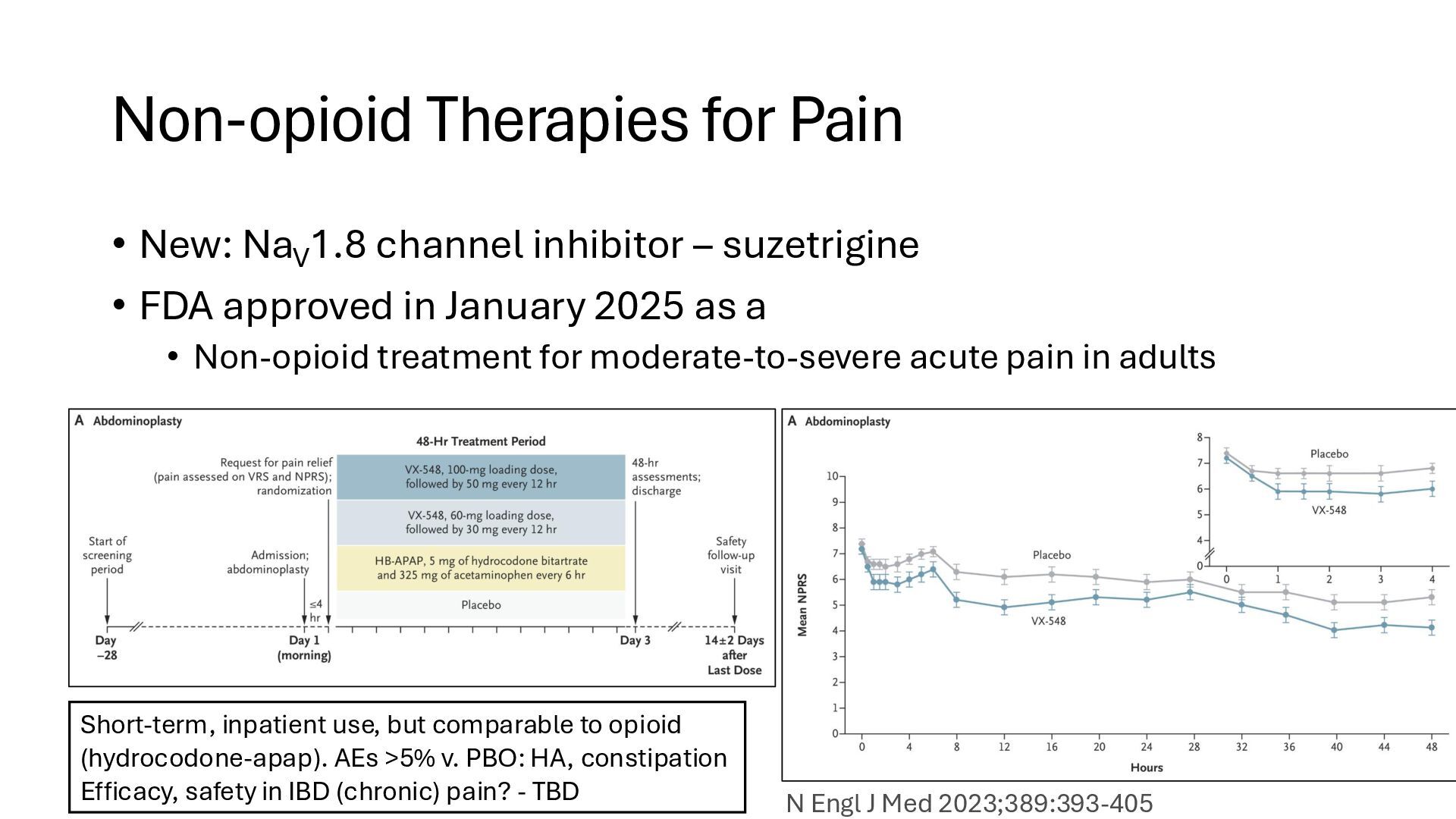
inhibitor – suzetrigine • FDA approved in January 2025 as a • Non-opioid treatment for moderate-to-severe acute pain in adults Short-term, inpatient use, but comparable to opioid (hydrocodone-apap). AEs >5% v. PBO: HA, constipation Efficacy, safety in IBD (chronic) pain? - TBD N Engl J Med 2023;389:393-405
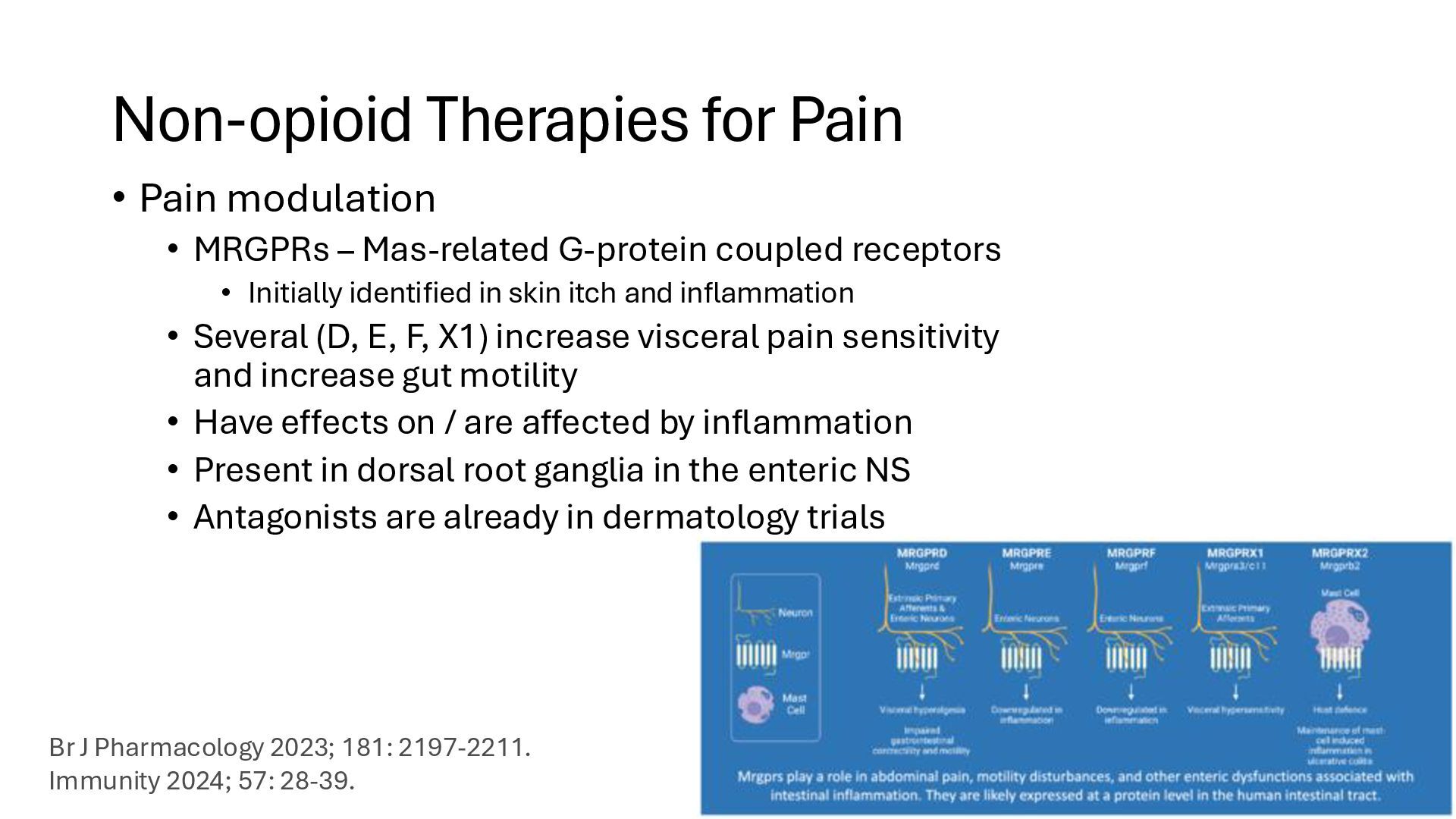
Mas-related G-protein coupled receptors • Initially identified in skin itch and inflammation • Several (D, E, F, X1) increase visceral pain sensitivity and increase gut motility • Have effects on / are affected by inflammation • Present in dorsal root ganglia in the enteric NS • Antagonists are already in dermatology trials Br J Pharmacology 2023; 181: 2197-2211. Immunity 2024; 57: 28-39.
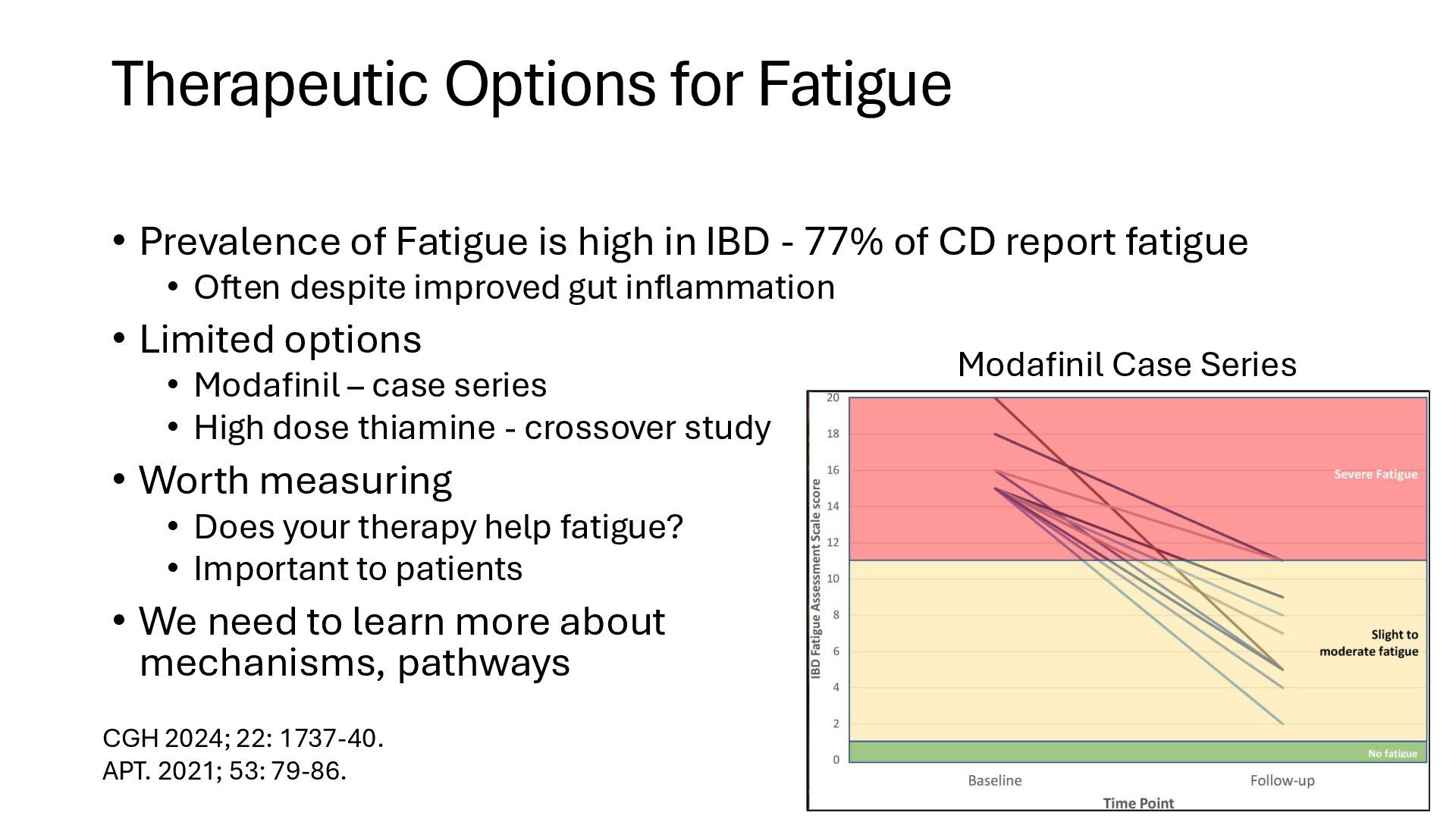
in IBD - 77% of CD report fatigue • Often despite improved gut inflammation • Limited options • Modafinil – case series • High dose thiamine - crossover study • Worth measuring • Does your therapy help fatigue? • Important to patients • We need to learn more about mechanisms, pathways Modafinil Case Series CGH 2024; 22: 1737-40. APT. 2021; 53: 79-86.
high (42%) in IBD • Why is this? • Psychological trauma? • Subclinical inflammation? • Hormone effects? • Deficiencies (choline)? • Worth measuring, possibly targeting • Does your therapy improve concentration? • Important to patients
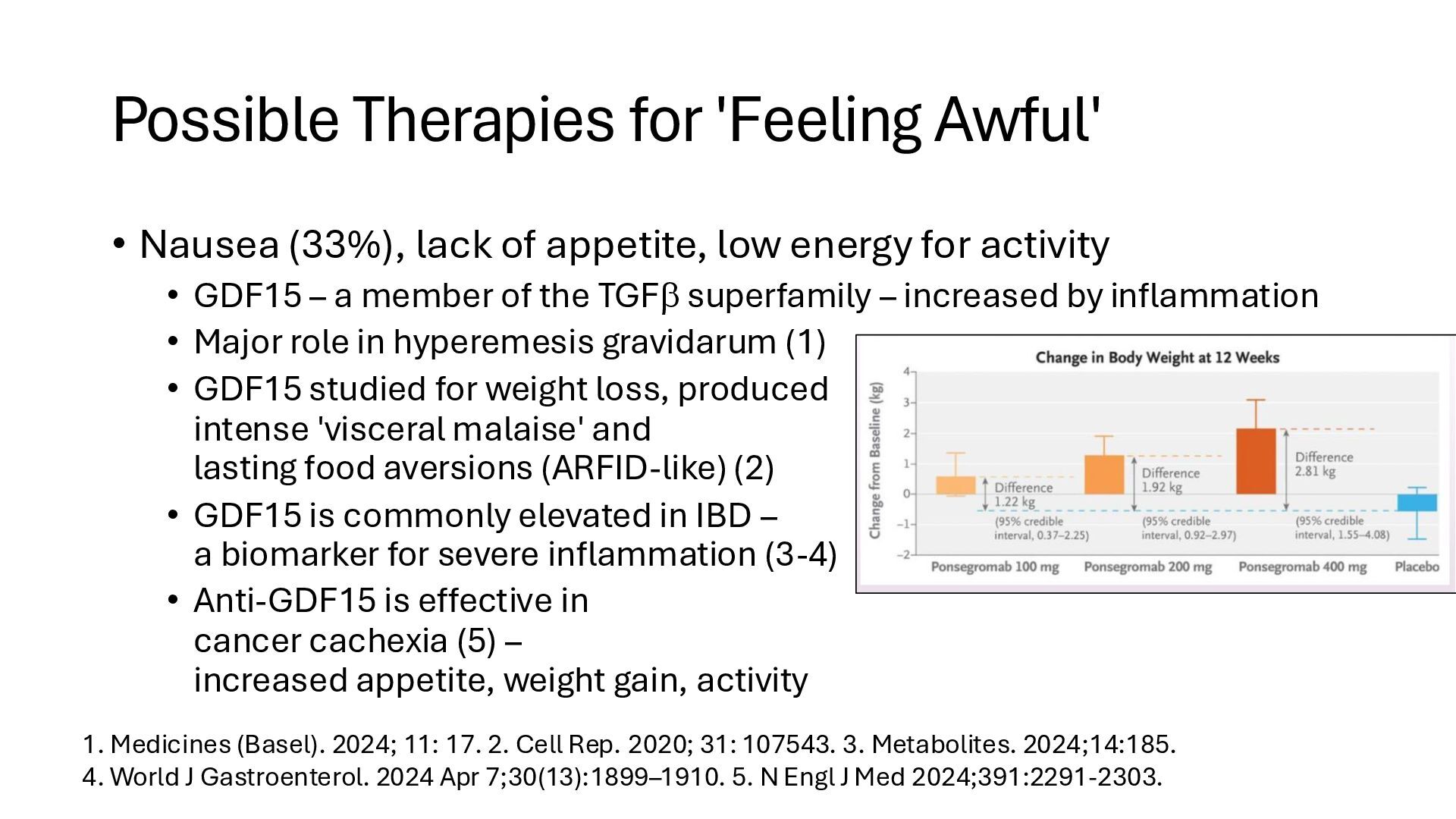
appetite, low energy for activity • GDF15 – a member of the TGF superfamily – increased by inflammation • Major role in hyperemesis gravidarum (1) • GDF15 studied for weight loss, produced intense 'visceral malaise' and lasting food aversions (ARFID-like) (2) • GDF15 is commonly elevated in IBD – a biomarker for severe inflammation (3-4) • Anti-GDF15 is effective in cancer cachexia (5) – increased appetite, weight gain, activity 1. Medicines (Basel). 2024; 11: 17. 2. Cell Rep. 2020; 31: 107543. 3. Metabolites. 2024;14:185. 4. World J Gastroenterol. 2024 Apr 7;30(13):1899–1910. 5. N Engl J Med 2024;391:2291-2303.
(but the ceiling is too low) • Durability gap – where is the 40-year dream? • Gaps in fistulizing disease and fibrosis – structural problems • Gaps in barrier boosting – can we speed healing? Prevent flares? • Novel strategies – monitor and intervene very early, biologics when smoldering, cell therapies curative(?), ADCs, microbiome • Gaps in addressing symptoms: pain, fatigue, concentration difficulties, nausea
PROs • Role of inflammation/sensitization vs fibrosis/rectal compliance • Floor effect on daily BMs in trials • The burgundy vs. champagne flute rectum
Local control of inflammation (tofacitinib suppositories) • Local reduction of sensitization (benzos/bentyl supp) • MRGPR antagonists? • Fibrosis / Compliance pathway • Treat fibrosis / wall thickening • Agents to increase compliance? • Targeted version of peppermint oil? • Identify the actual target (TRPM8, TRPA1?) • Make a better mousetrap
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}