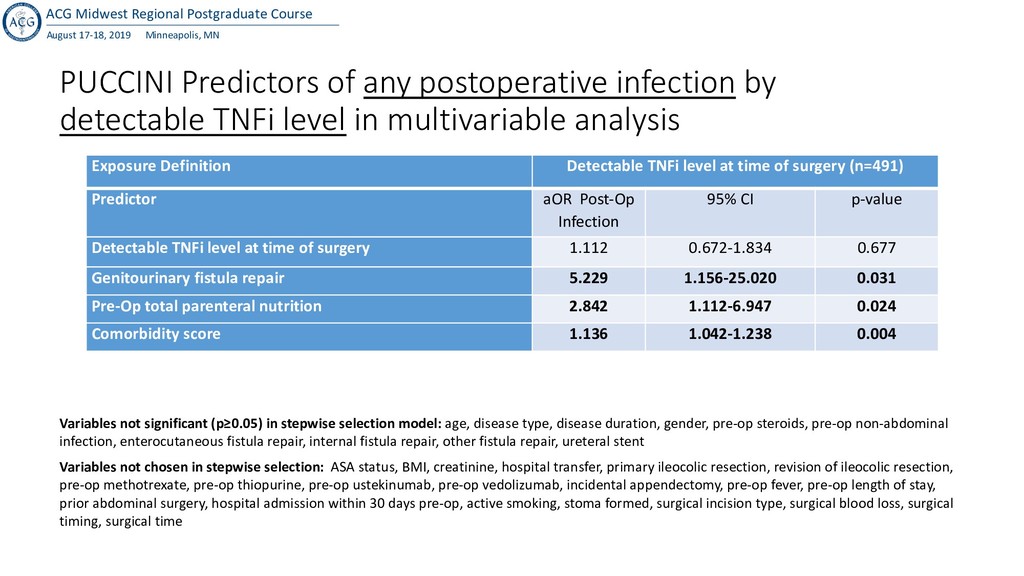
PUCCINI Predictors of any postoperative infection by detectable TNFi level in multivariable analysis Exposure Definition Detectable TNFi level at time of surgery (n=491) Predictor aOR Post-Op Infection 95% CI p-value Detectable TNFi level at time of surgery 1.112 0.672-1.834 0.677 Genitourinary fistula repair 5.229 1.156-25.020 0.031 Pre-Op total parenteral nutrition 2.842 1.112-6.947 0.024 Comorbidity score 1.136 1.042-1.238 0.004 Variables not significant (p≥0.05) in stepwise selection model: age, disease type, disease duration, gender, pre-op steroids, pre-op non-abdominal infection, enterocutaneous fistula repair, internal fistula repair, other fistula repair, ureteral stent Variables not chosen in stepwise selection: ASA status, BMI, creatinine, hospital transfer, primary ileocolic resection, revision of ileocolic resection, pre-op methotrexate, pre-op thiopurine, pre-op ustekinumab, pre-op vedolizumab, incidental appendectomy, pre-op fever, pre-op length of stay, prior abdominal surgery, hospital admission within 30 days pre-op, active smoking, stoma formed, surgical incision type, surgical blood loss, surgical timing, surgical time
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}